 Vascular access is the Achilles tendon of hemodialysis. Just yesterday, I saw a patient with one of those lumbar catheters… Examining his arm revealed that he had failed 4 attempts of access creation (2 fistulas and 2 grafts). With that in mind, let’s start by reviewing the key components for a successful AVF creation: in our hospital, evaluation before placement of a fistula starts with:
Vascular access is the Achilles tendon of hemodialysis. Just yesterday, I saw a patient with one of those lumbar catheters… Examining his arm revealed that he had failed 4 attempts of access creation (2 fistulas and 2 grafts). With that in mind, let’s start by reviewing the key components for a successful AVF creation: in our hospital, evaluation before placement of a fistula starts with:
*Dopplers of the upper extremities.
*The arterial lumen should have > 2.0mm at the point of anastomosis and the venous side should be at least 2.5mm.
*Ensuring that there are no proximal venous stenosis is also key, since some patients had lines before that increases the risk of subclavian stenosis, leading to inadequate maturation of the access.
Many of the diabetic patients have very small vessels, creating a special challenge for fistula maturation.
The order of preference for AVF creation once vessel size is confirmed is the following:
- radial-cephalic
- brachial-cephalic
- brachial-basilic transposition.
Once the AVF is created, the rule of 6 apply in order to decide about usage (as discussed by Nate).
6 weeks after the AV fistula has been placed, the fistula should:
(a) be able to support a blood flow of 600 ml/min.
(b) be at a maximum of 6mm from the surface.
(c) have a diameter greater than 6mm.
There are multiple reasons for a fistula not to mature, but the main causes of early fistula failure can be classified as:
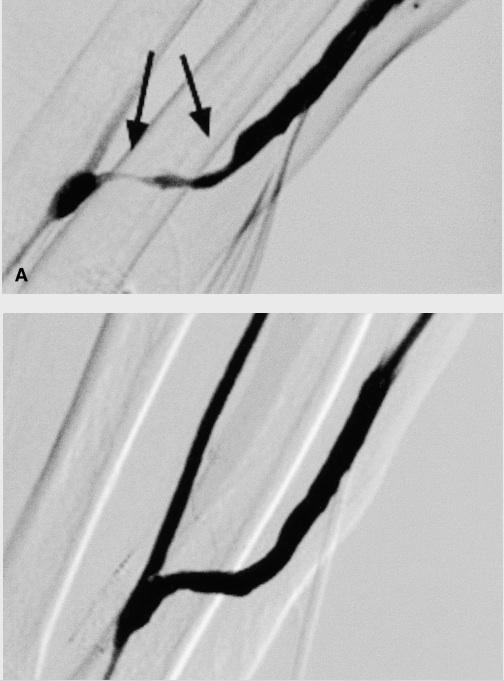
Inflow problems: pre-existing arterial anomalies (anatominally small, atherosclerotic disease) or acquired (juxta-anastomototic stenosis)
Outflow problems: pre-existing venous anomalies like anatomically small, fibrotic vein, proximal venous stenosis and accessory veins.


one more point i would like to add here is, there are some centres which start of with snuff box fistula esp in young, non diabetics…..
Any thoughts about exercising the arm prior to AV placement as well as post access placement?
Hi Yudi, dopplers are used before fistula placement in the evaluation of the vessels size. Once you have a fistula that is not maturing, fistulogram is the gold standard since it can be both diagnostic and therapeutic. I do believe angioplasty can help maturation in some cases, but I still think outcomes are less than optimal.
Agreed about rule of 6 and that the AV access is the achilles heel of hemodialysis.
However I disagree regarding doppler use. If the fistula can't be used in 6 weeks, best to just plasty imho.
Any comments on using ballon assisted maturation of fistulas? Something I'm trying at the moment