POCUS = Point-of-Case Ultrasound POCUN = Point-of-Care Ultrasound in Nephrology RFN Focus on POCUN Series
Kidney
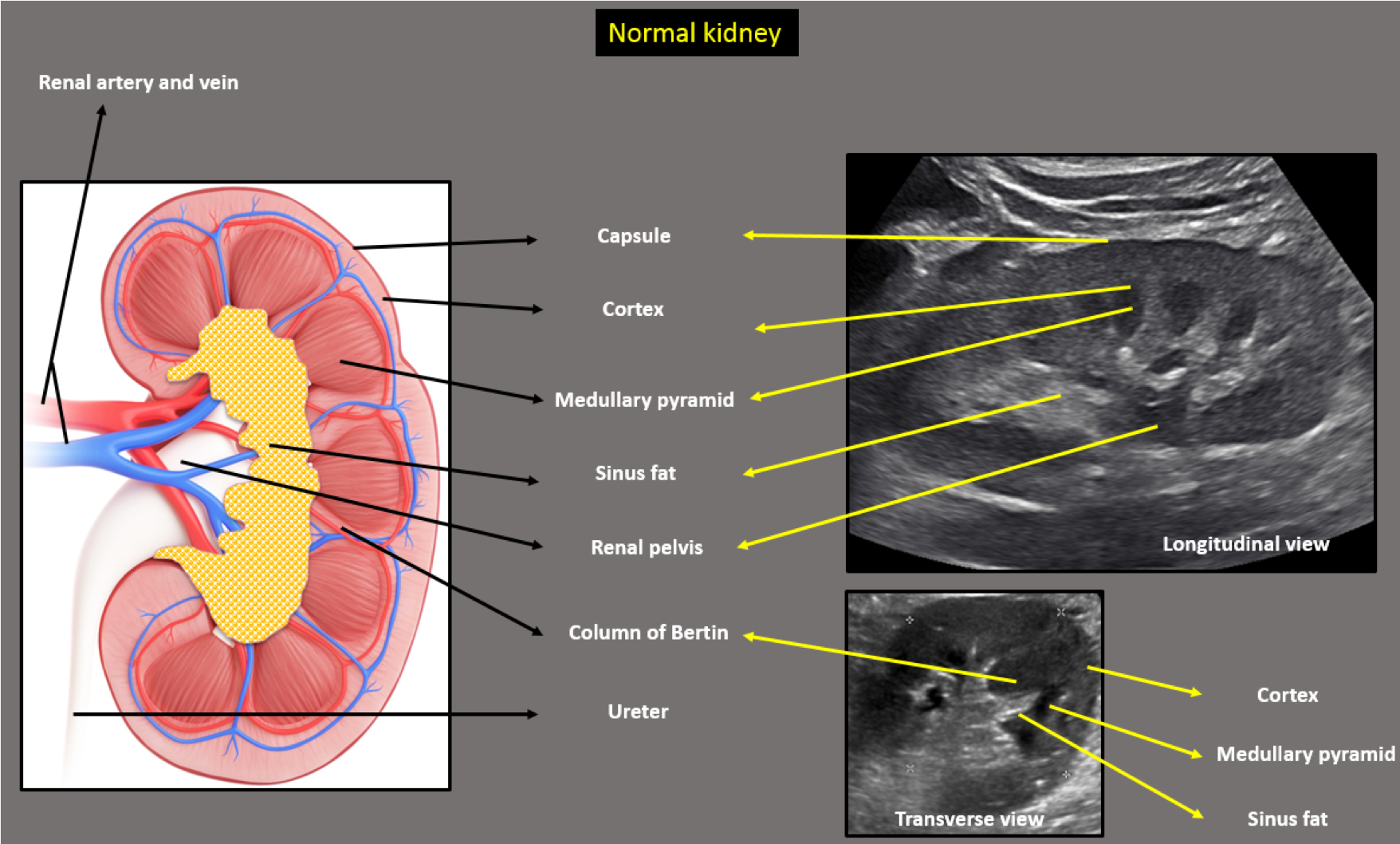
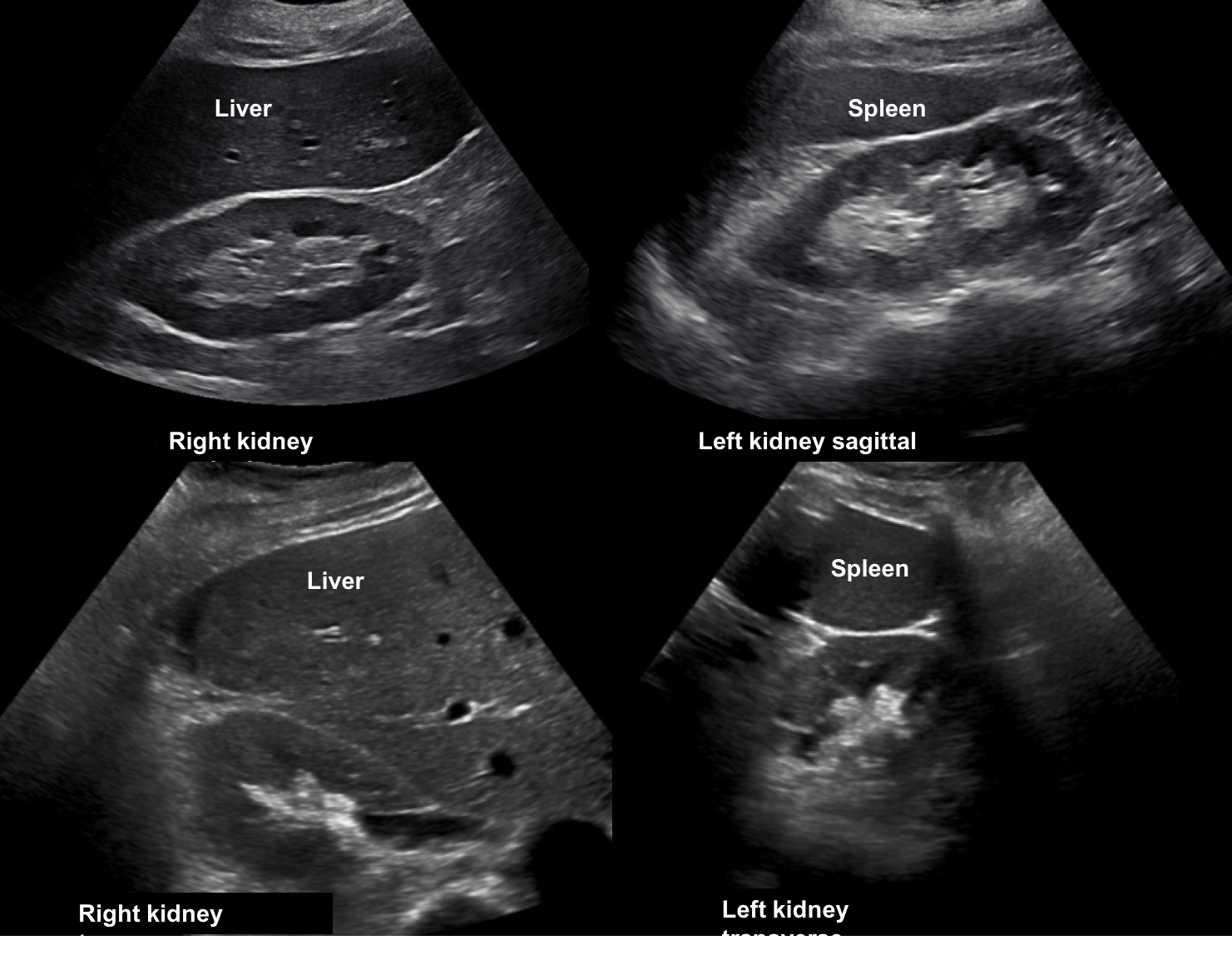
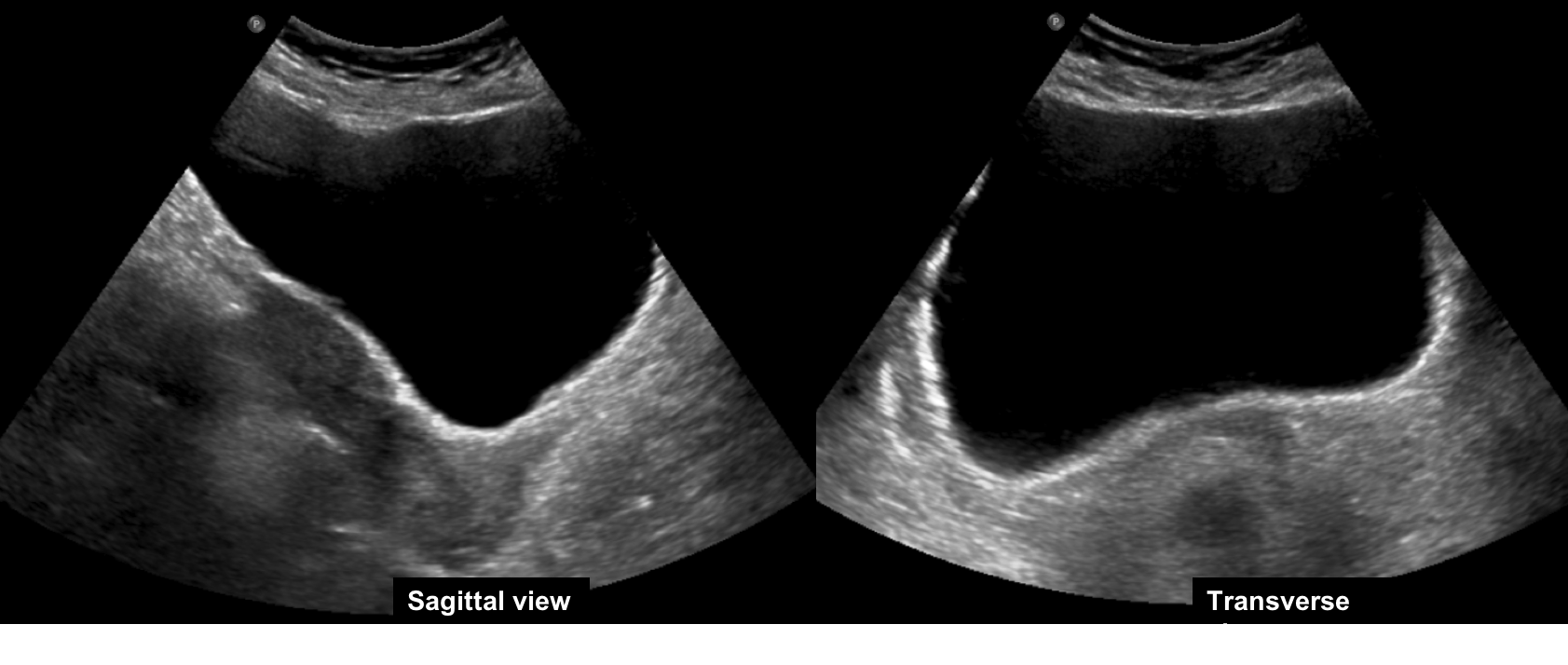
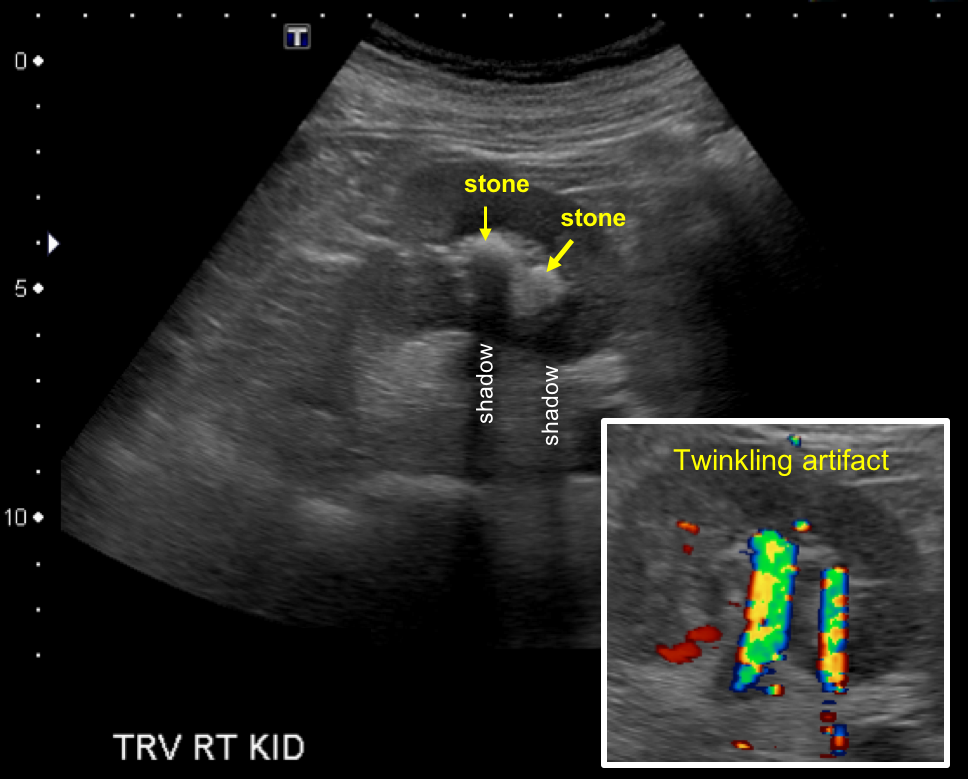
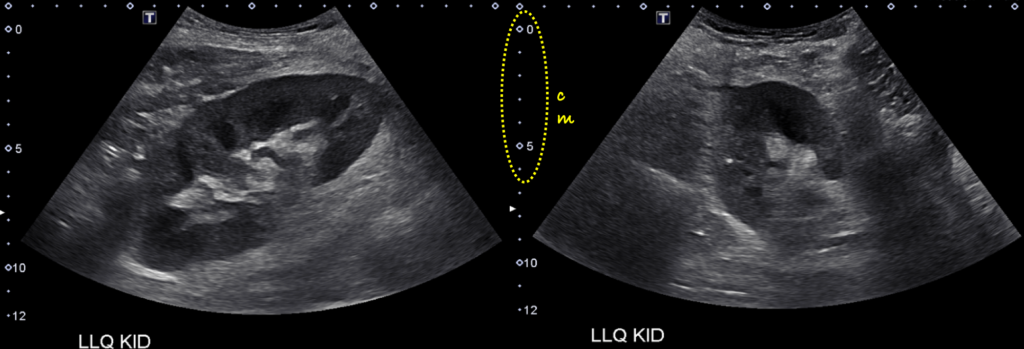
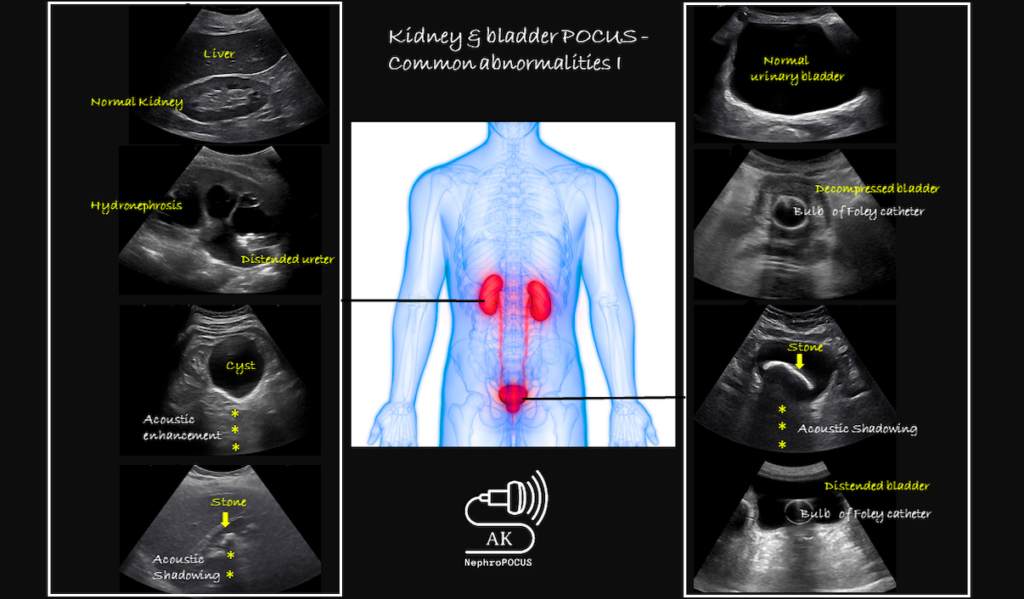
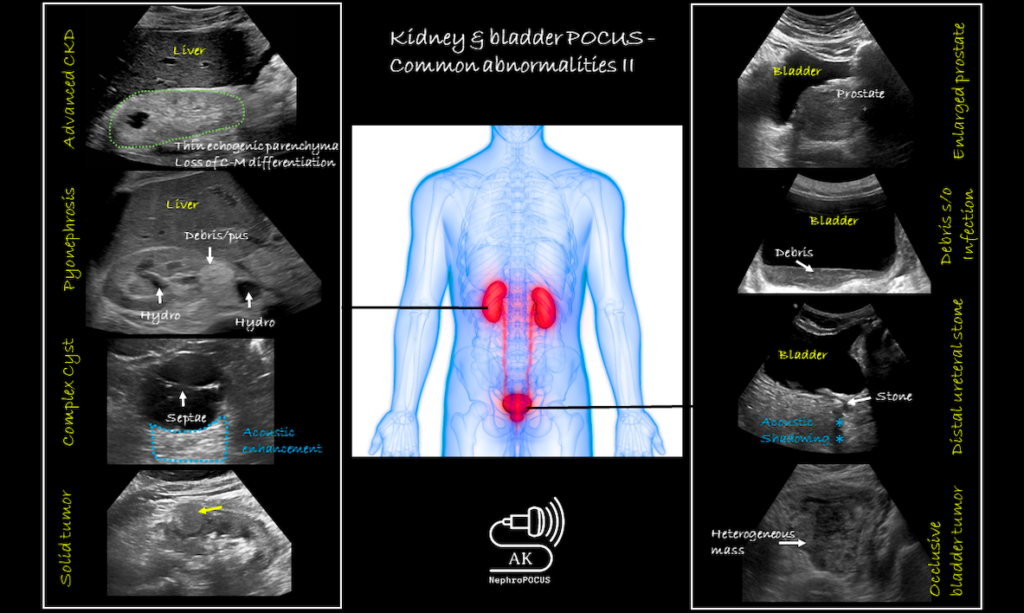
Normal Kidney. The echogenic capsule makes the bean shaped organ easily identifiable. The cortex is either isoechoic or hypoechoic (more commonly) compared with the normal liver or normal spleen. The medullary pyramids are hypoechoic or anechoic compared to cortex. On most occasions, the pyramidal shape is not well visualized. The renal cortical tissue extends into the medulla, separating pyramids in the form of columns called ‘columns of Bertin’. Renal sinus fat is echogenic and occupies major part of the inner kidney. The collecting system is usually not visualized unless distended and is embedded in the surrounding echogenic sinus fat. The renal pelvis area is hypoechoic but not “black” unless there is hydronephrosis. Similarly, ureters are not seen unless distended (hydroureter). Normal Kidney. Sagittal and transverse views, liver on the right and spleen on the left. Normal Urinary Bladder. It appears as an anechoic fluid-filled structure (urine is black on ultrasound) located in the mid pelvis. A full bladder is necessary to comprehensively evaluate the characteristics of its walls, contents and pelvic organs. The sagittal view is triangular and transverse section is rectangular – but the shape varies depending on bladder fullness. Kidney Stones. On grey scale image, stones appear as hyperechoic or bright structures with a posterior “acoustic shadow.” Acoustic shadowing is the black or anechoic area seen beyond structures that do not transmit ultrasound waves. In the Doppler view (inset), stones exhibit a “twinkling sign” or artifact – rapidly alternating focus of color Doppler signals mimicking turbulent flow . This artifact is more pronounced with rougher stones, and more sensitive than shadowing for detection of small stones. Cysts. A.Simple cyst: well-defined, round, anechoic structure. Increased through transmission manifested by “acoustic enhancement”, which refers to the increased intensity of echoes (bright area) relative to surrounding tissues, distal to a structure that transmits the sound waves very well. B. Large kidney with multiple cysts, seen in Autosomal dominant polycystic kidney disease. C. Complex cyst with internal septations. Hydronephrosis.A. Mild hydronephrosis: dilatation of the renal pelvis and calyces with preserved pelvicalyceal pattern. Cortico-medullary differentiation is preserved and we can see the pyramids. B. Moderate hydronephrosis: As the severity of hydronephrosis increases, urine moves proximally into the kidney exerting pressure on the parenchyma. There is increasing dilatation of the renal pelvis and urine extending inside the kidney. The convex irregular border of the collecting system at the top mimics a “cauliflower appearance.” C. Severe hydronephrosis: renal pelvis and calyces appear ballooned and cortico-medullary differentiation is lost, making the cortex thin. The kidney looks like a fluid filled bag. Normal Kidney Transplant. The image demonstrates a normal left lower quadrant renal allograft. Transplanted kidney essentially looks the same as native kidney on a sonogram except for its superficial location (note the depth from skin surface on the scale) and that no associated liver or spleen will be seen in the image.
Kidney Transplant
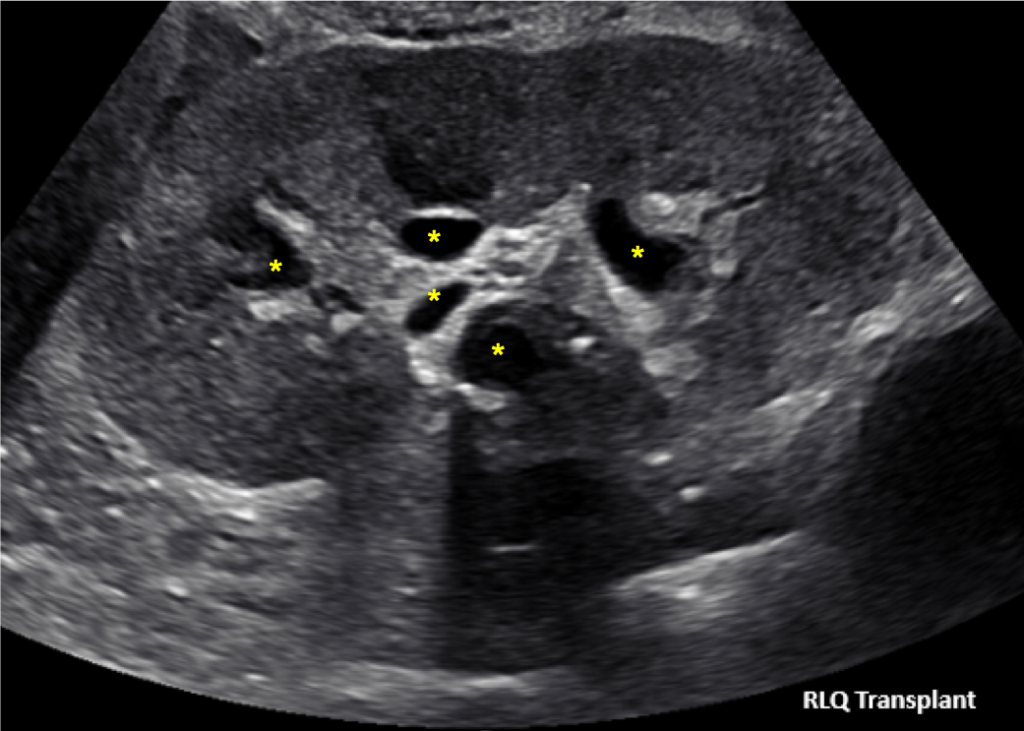
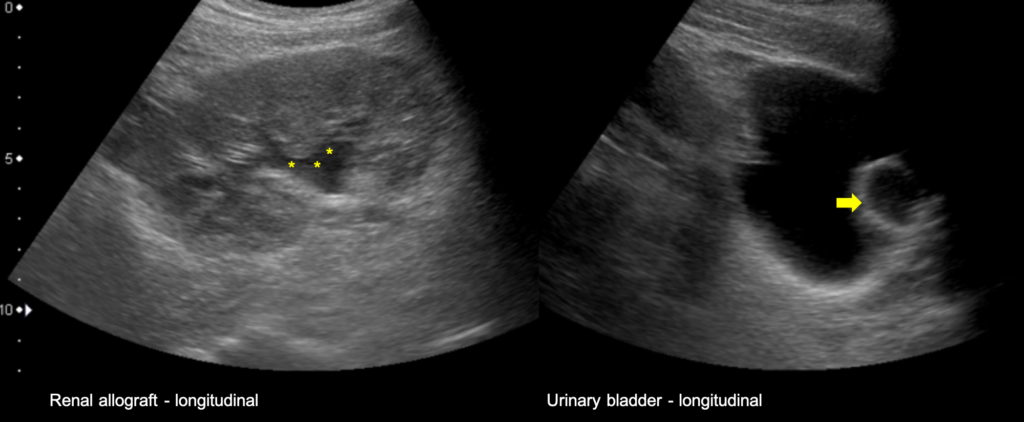
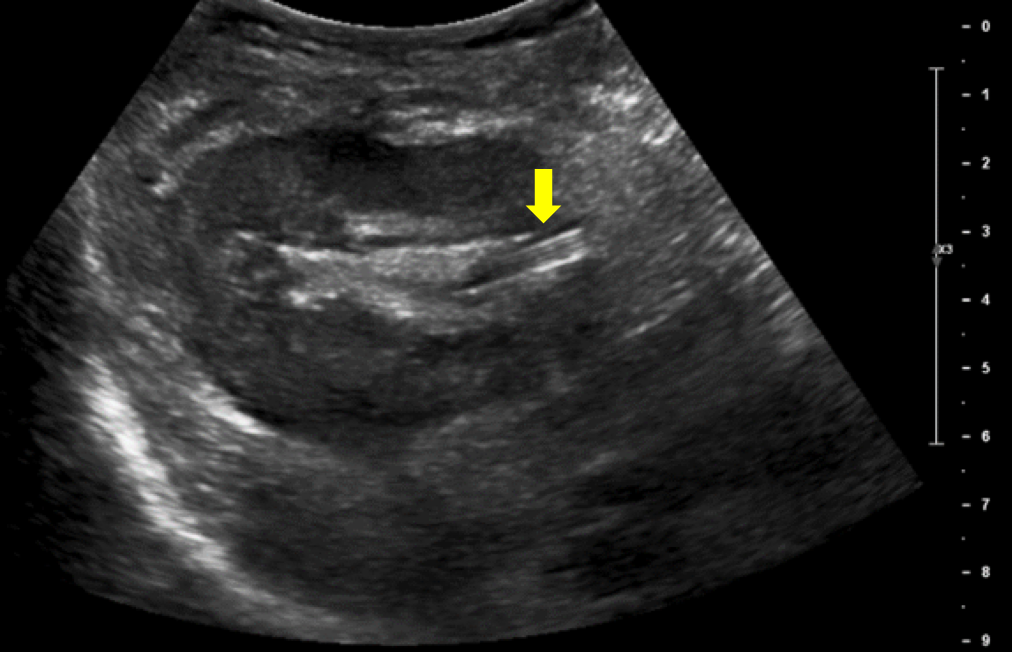
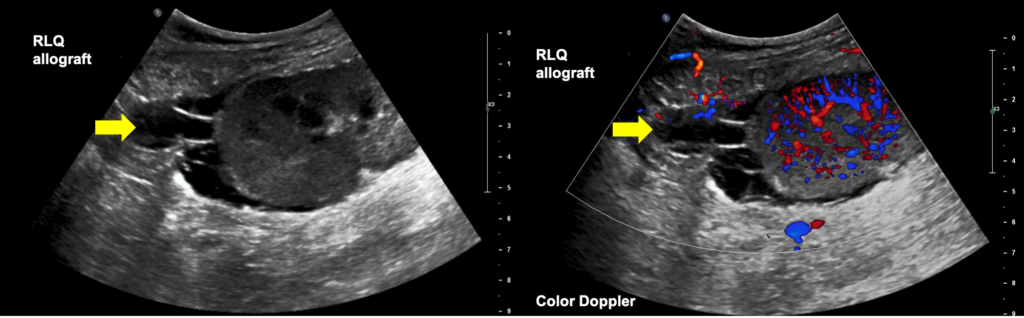
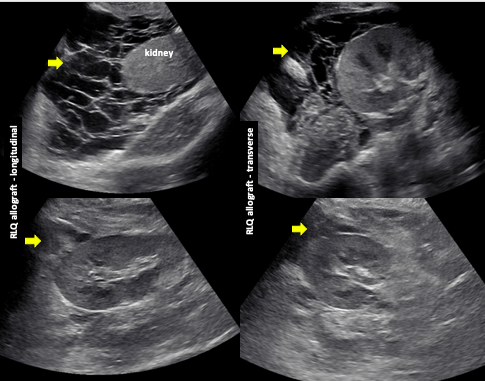
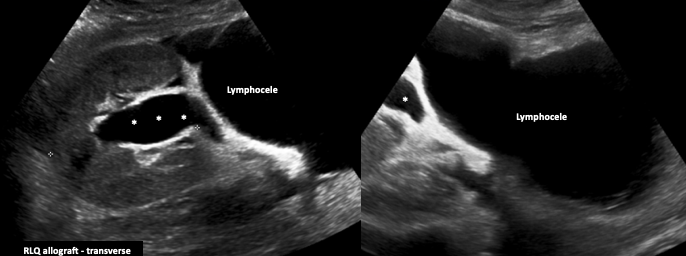
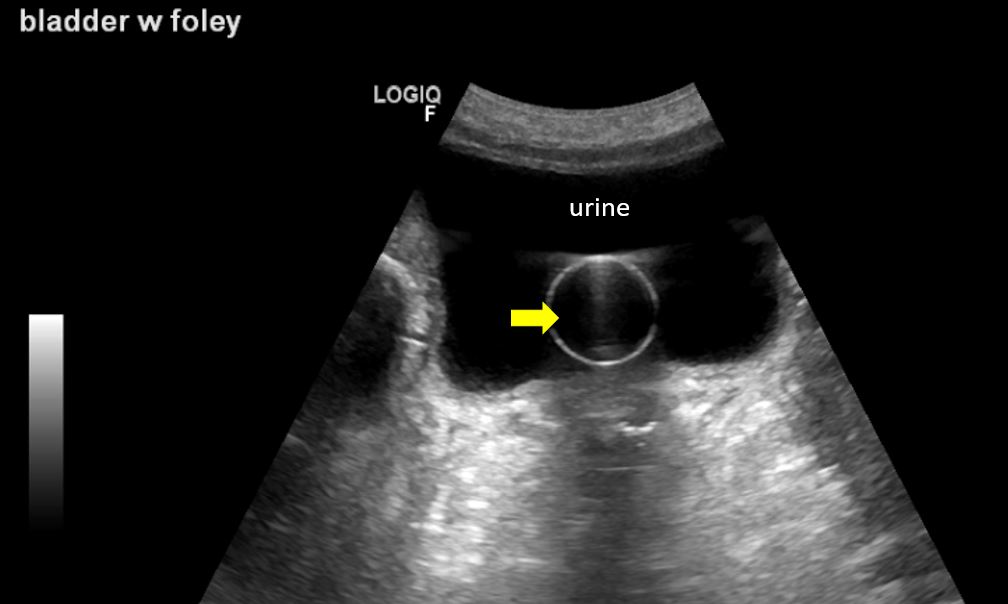
Normal KidneyTransplant. Normal allograft with slightly distended pelvicalyceal system (indicated with asterisks). Note that the collecting system of a well-functioning transplanted kidney is often slightly dilated, likely because of a combination of an increased volume of urine produced (i.e. acting as the sole kidney), loss of the ureter’s tonicity from denervation and altered anatomy of the ureterovesical junction due to surgery. Kidney allograft demonstrating mild dilatation of the pelvicalyceal system (asterisks). Before labeling it as an ‘expected’ finding, we need to do 2 things: 1st: compare with prior imaging. This patient did not have this dilated collecting system a month prior. 2nd: scan the bladder. In this case, despite the presence of Foley catheter (arrow points to Foley balloon), the bladder is distended with urine (black thing surrounding the balloon) which is suggestive of obstructive Foley as the cause for the collecting system dilatation. New renal transplant demonstrating ureteral stent (arrows). Stent appears as a hyperechoic tubular structure starting in the collecting system of the kidney and is not always traceable up to the urinary bladder. Changing the angle of insonation (looking from a different transducer angle) helps if the stent is not visible at first glance. Hematoma in Transplanted Kidney. One-month old renal transplant demonstrating a loculated fluid collection at the superior pole suggestive of hematoma. Fresh blood is anechoic and clotted blood appears hyperechoic on ultrasound. Hematomas typically don’t demonstrate Doppler flow because the blood is not flowing. Septated fluid around Kidney Transplant. [Top panel] Right lower quadrant transplanted kidney demonstrating a large collection of septated fluid around it. [Bottom panel] Substantial reduction in the perinephric collection can be seen status post evacuation. Lymphocele. Kidney allograft demonstrating a large lymphocele compressing the collecting system leading to hydronephrosis (asterisks).
Hydronephrosis
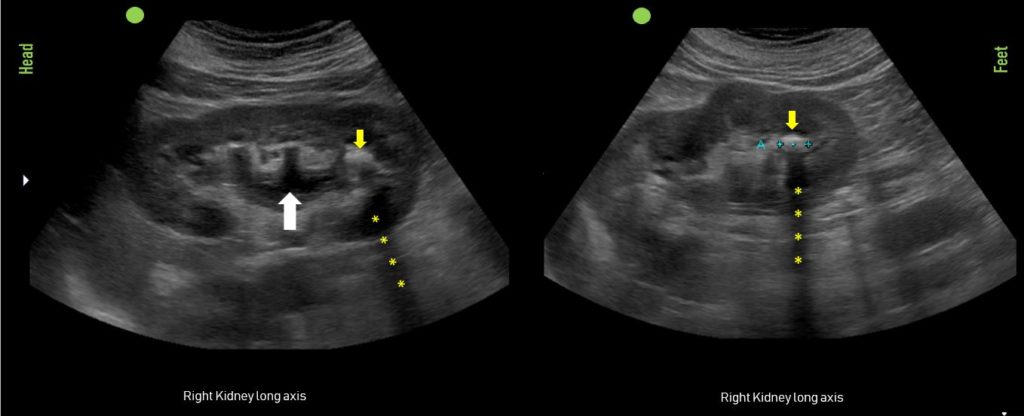
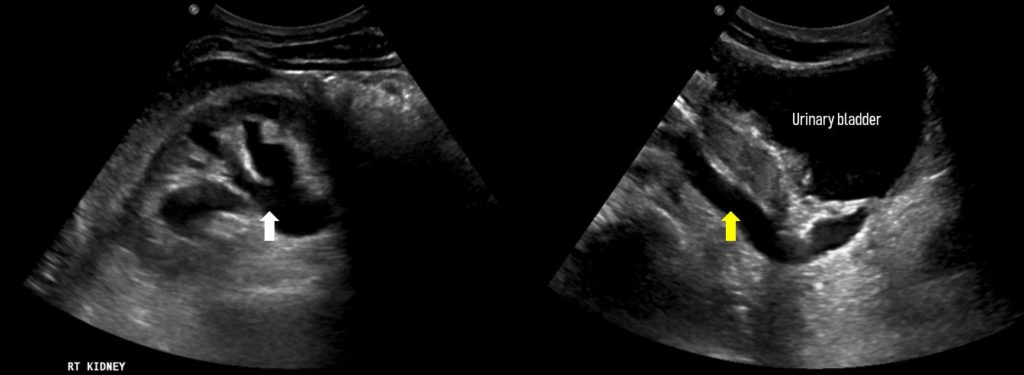
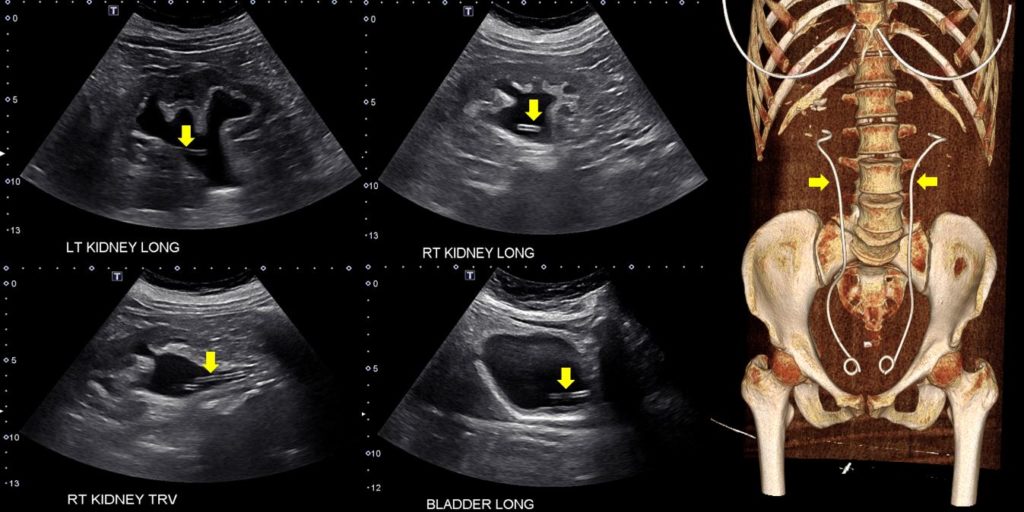
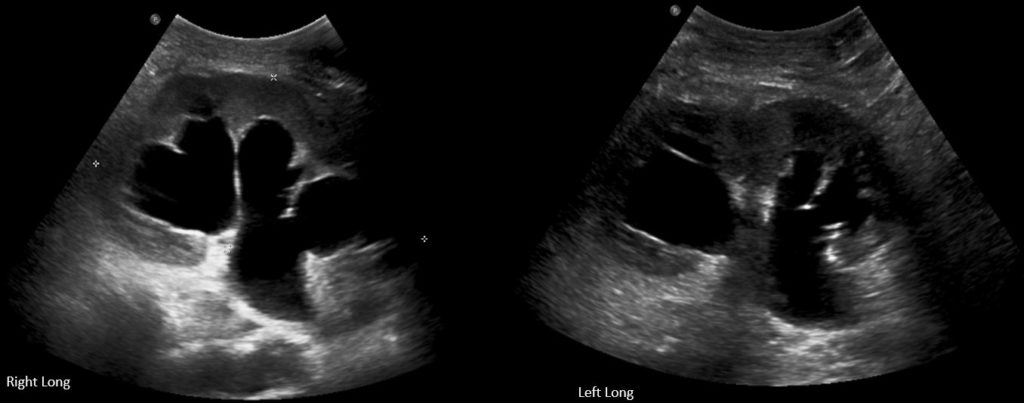
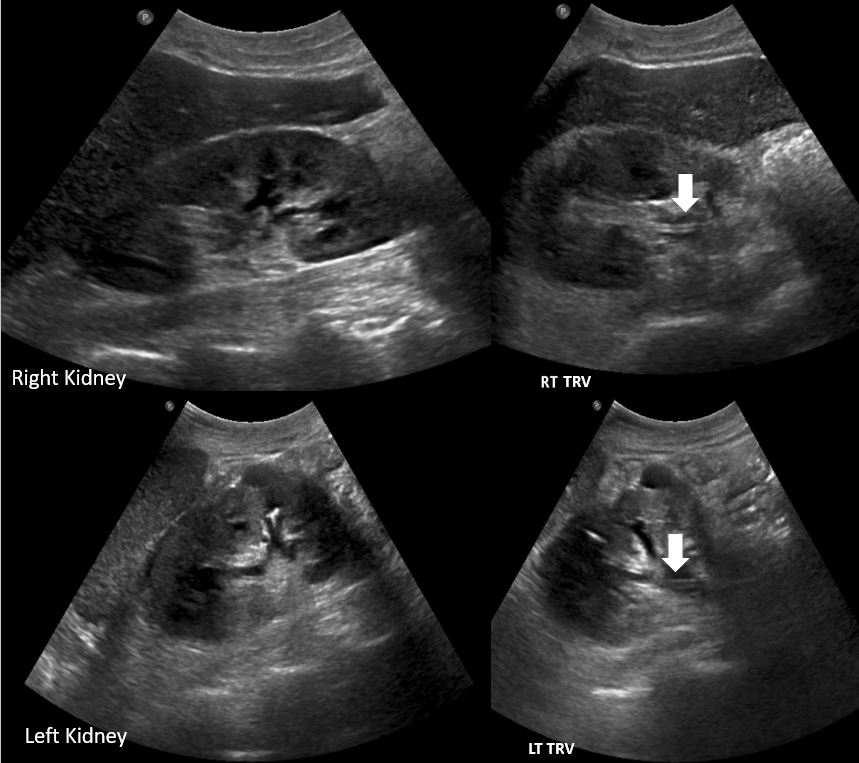
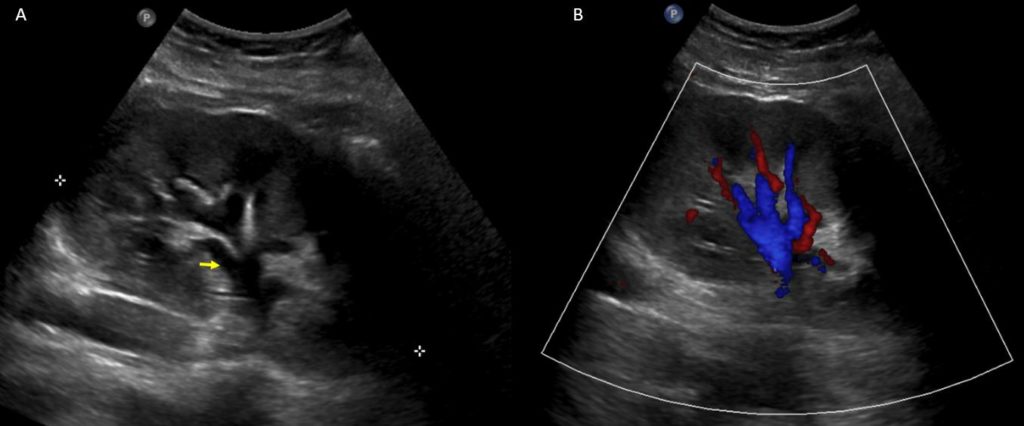
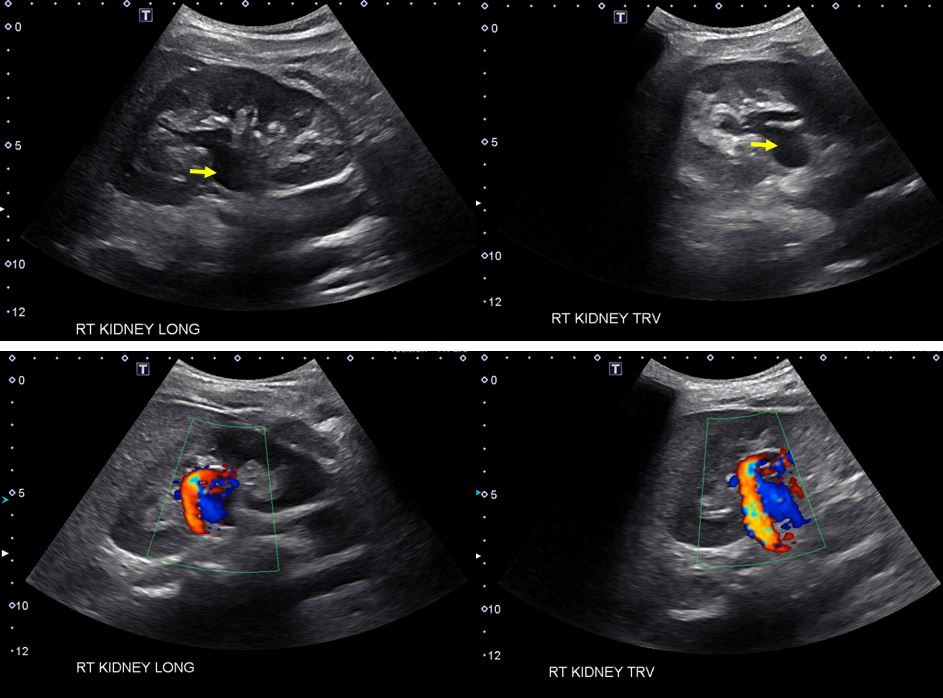
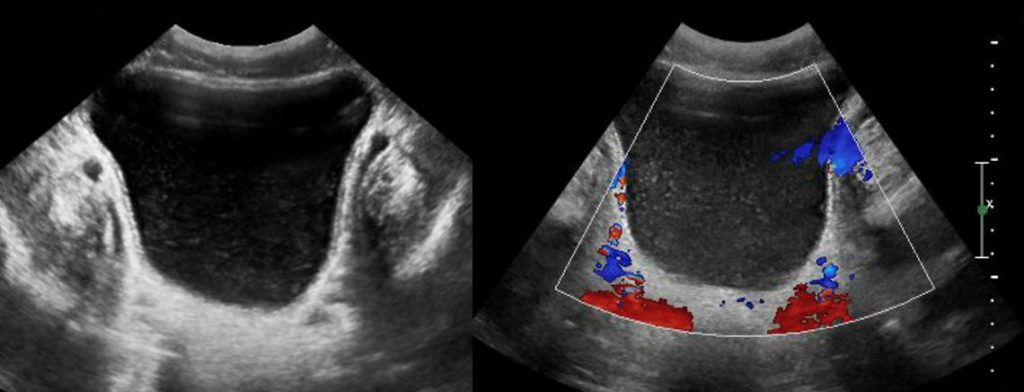
Mild hydronephrosis of the right kidney (white arrow). A stone (yellow arrow) with acoustic shadowing (asterisks) can be seen in the lower pole. Note that mild hydronephrosis may not be apparent in all images, which is why it is important to fan through the entire longitudinal plane of the kidney. Moderate hydronephrosis of the right kidney with hydroureter. Dilated pelvicalyceal system is indicated with white arrow and ureter with yellow arrow. Remember that an undilated ureter is not usually visualized on renal sonogram. Moderate hydronephrosis of the right kidney demonstrating a ureteral stent (arrows), which appears as a hyperechoic tubular structure seen in the renal pelvis area and in the urinary bladder. A representative 3 dimensional CT scan image is shown on the right to illustrate the location of ureteral stents. Bilateral severe hydronephrosis in a patient with cervical cancer. Previous patient with near-complete resolution of hydronephrosis after stent placement. Stents (arrows) are better seen on transverse images. Another case of bilateral severe hydronephrosis. A urinary bladder stone with accompanying acoustic shadowing (asterisks) can be seen. Right hydroureter without significant hydronephrosis secondary to a stone in transit (stone not seen in the image).Pyonephrosis: Note the echogenic material or pus (yellow arrows) within the dilated collecting system (blue arrows). (A) Anechoic renal pelvis resembling mild hydronephrosis on grey scale image. (B) on color Doppler, the same area demonstrates prominent vessels. As blood and urine appear black on ultrasound, it’s important to differentiate one from the other using color Doppler. [Top Panel] Longitudinal and transverse gray‐scale renal ultrasound images demonstrating anechoic region in the mid‐kidney suggestive of hydronephrosis in a patient with microscopic hematuria. [Bottom panel] Color Doppler images demonstrating turbulent arteriovenous flow suggestive of vascular malformation. This patient subsequently underwent angiography and coil embolization.
Pelvic and Bladder Abnormalities
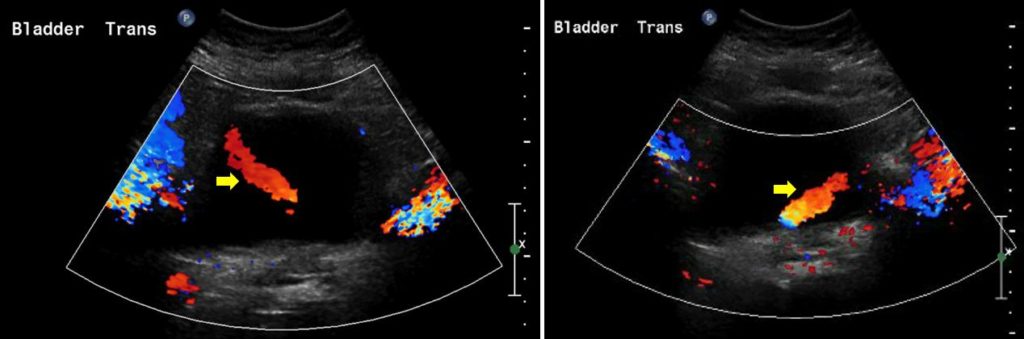
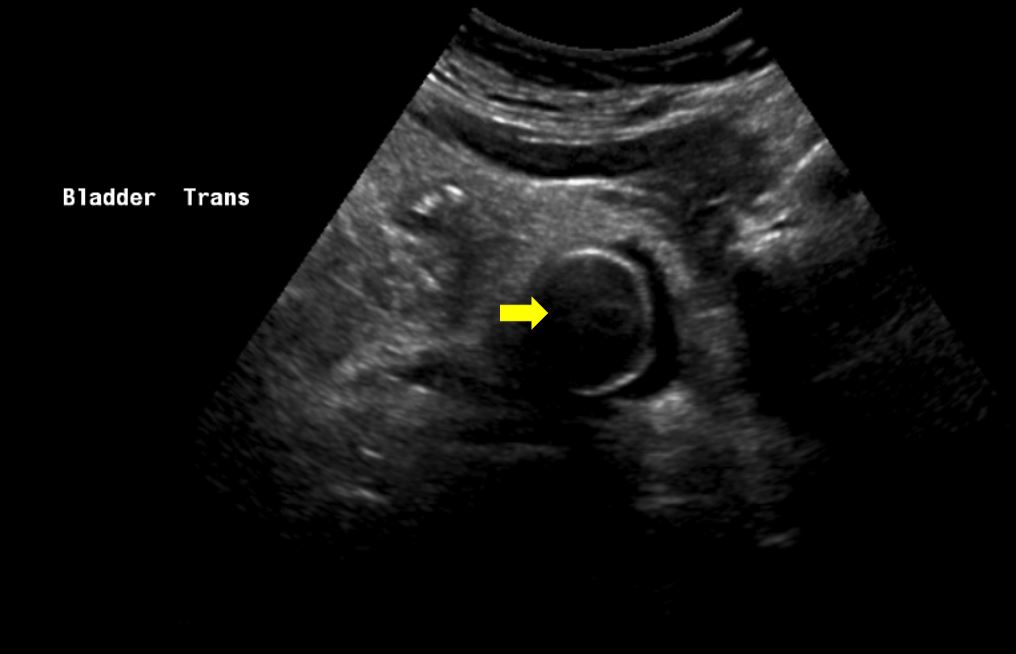
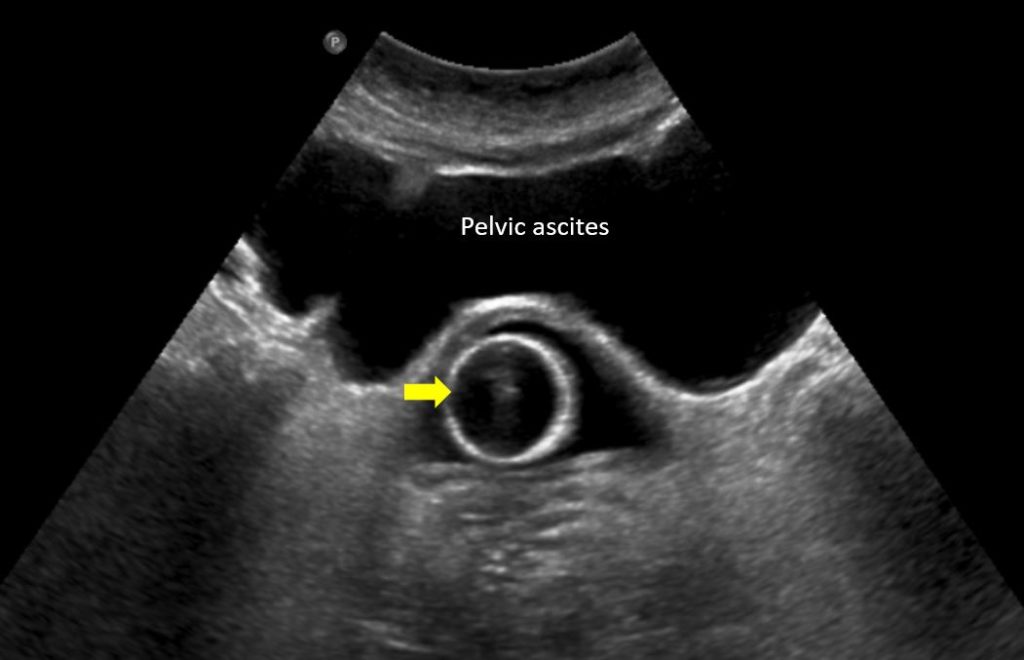
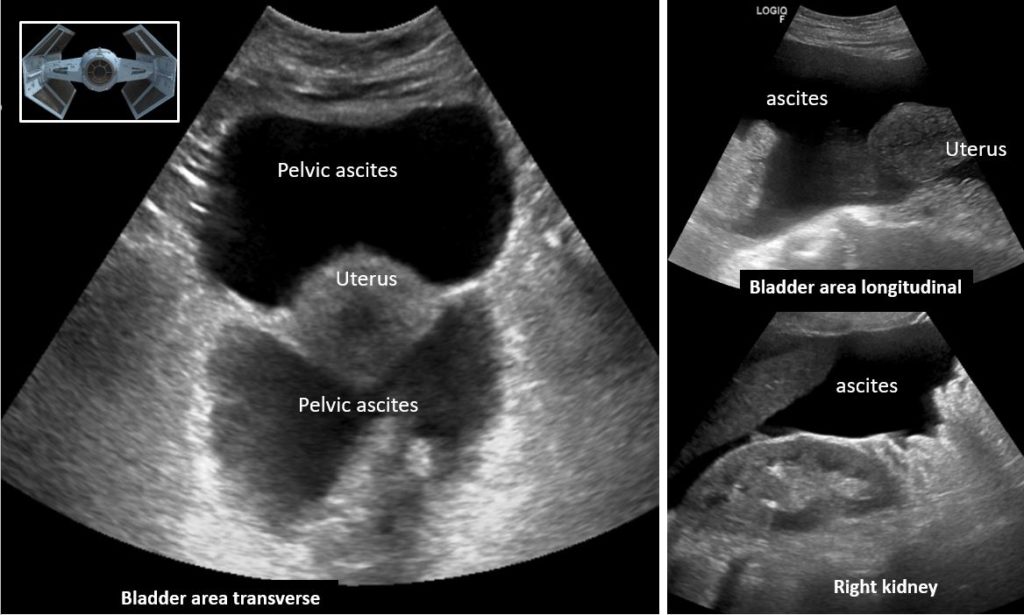
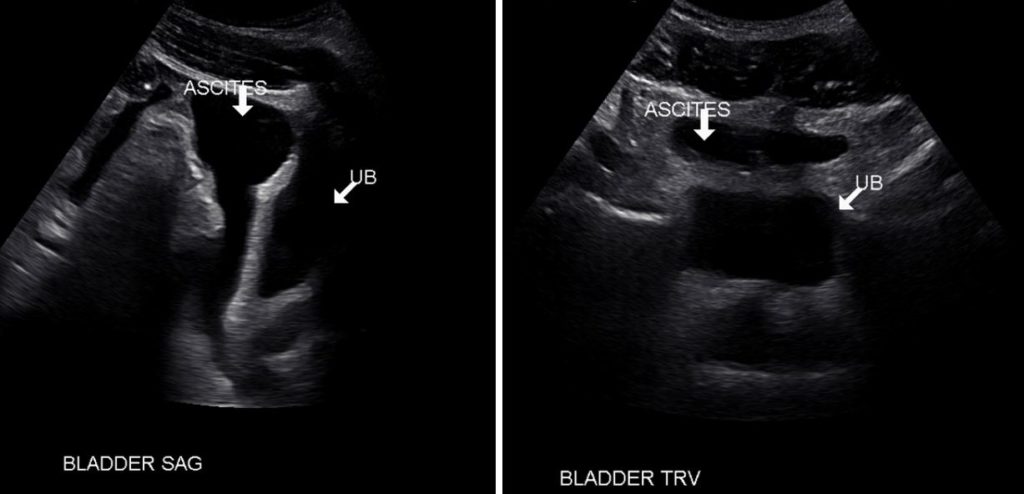
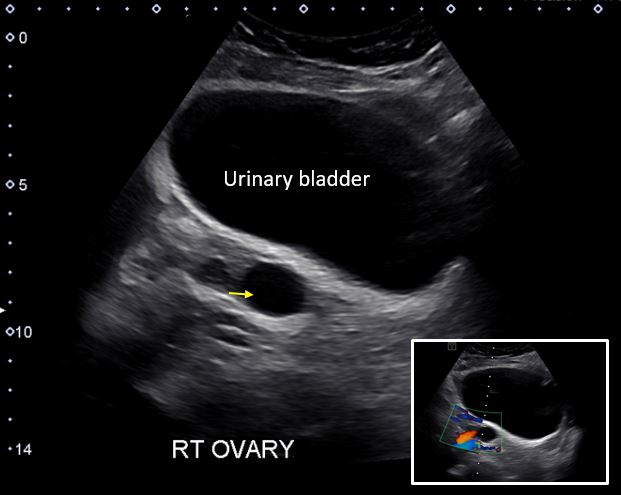
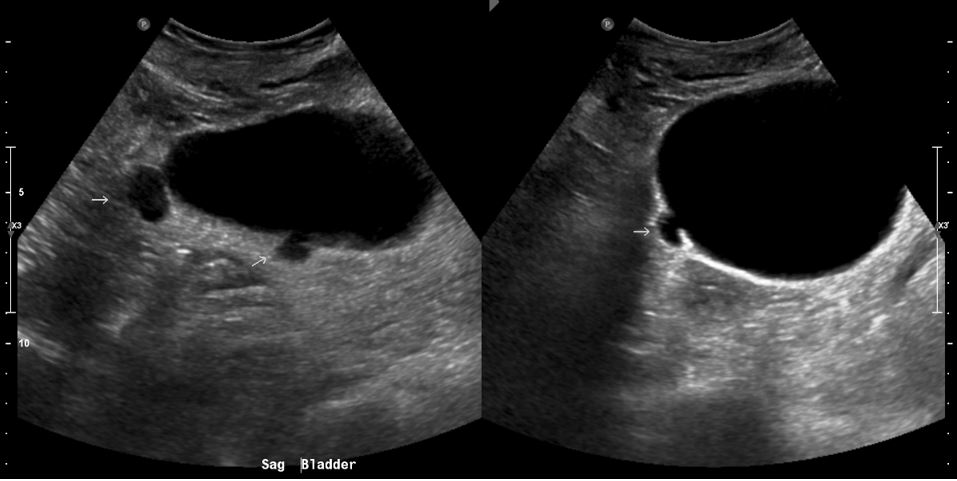
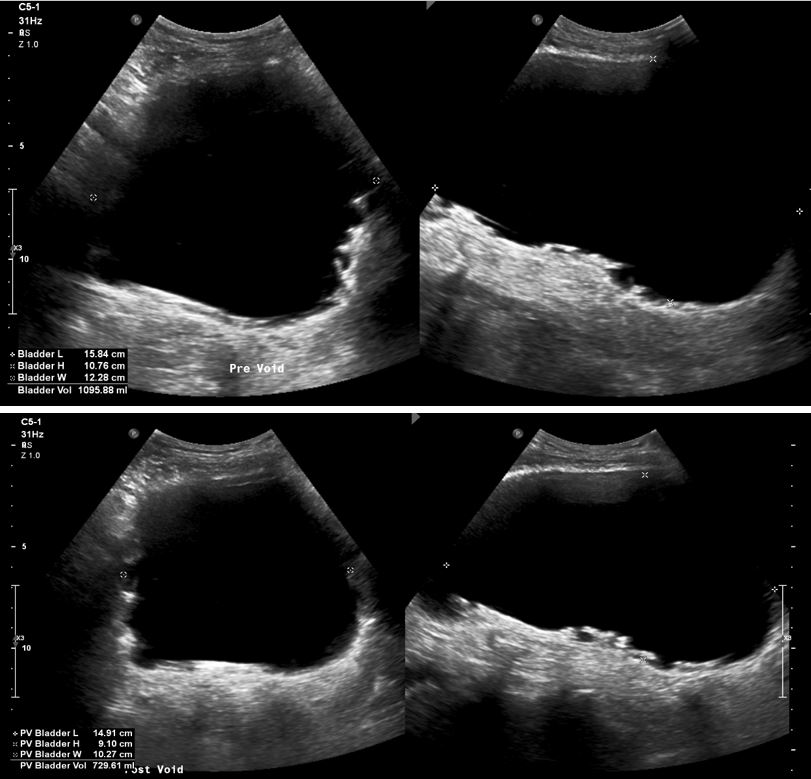
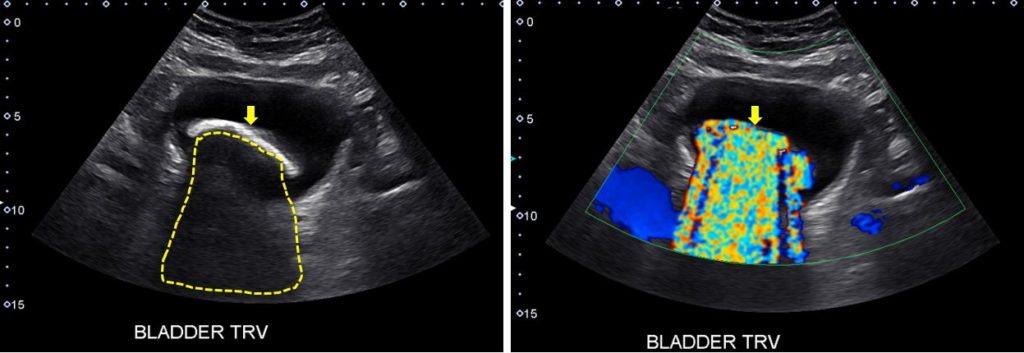
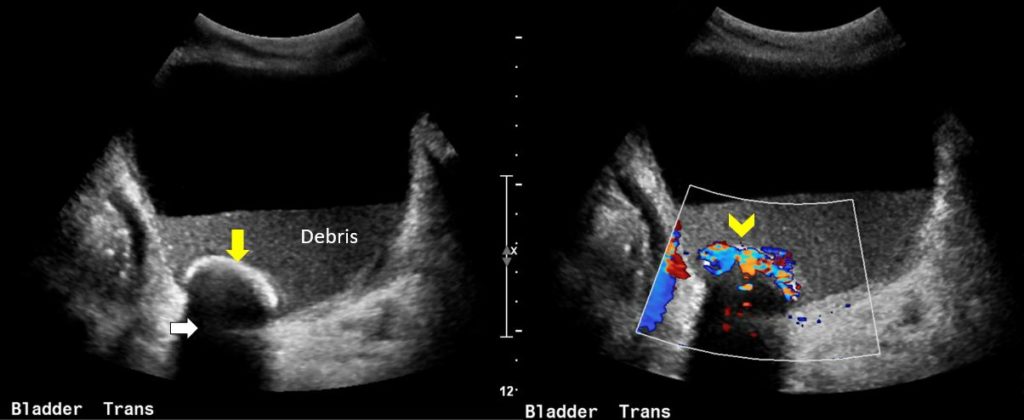
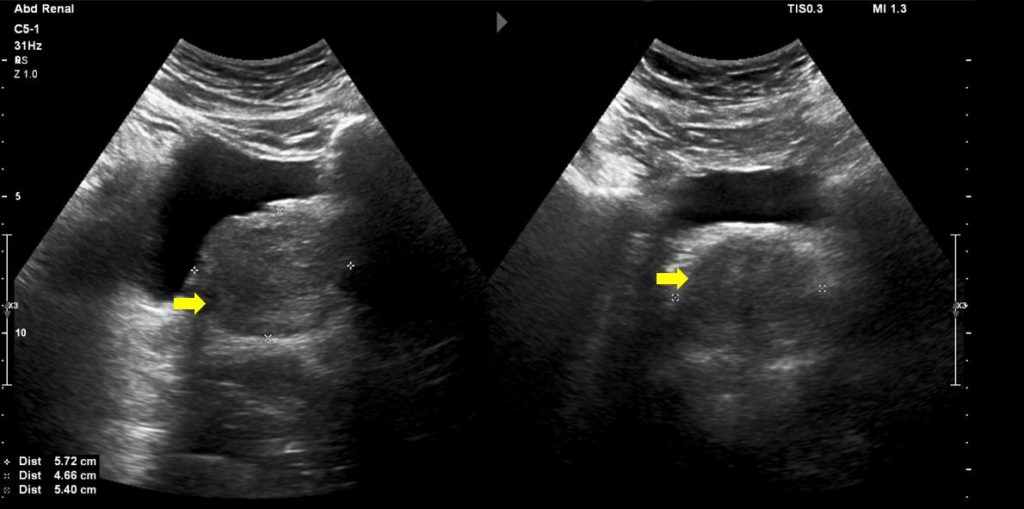
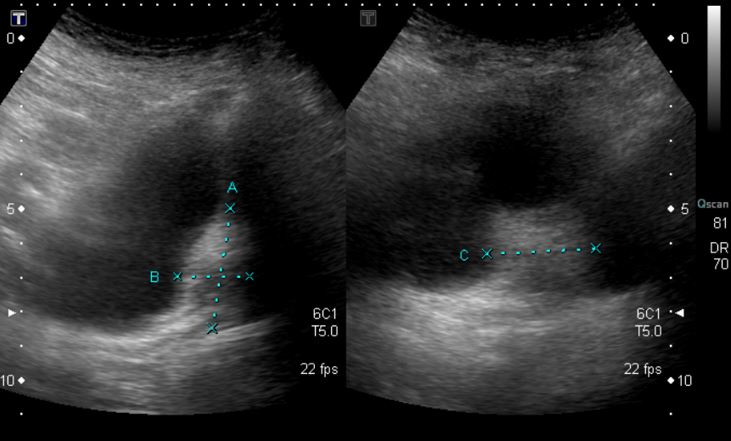
The image demonstrates right and left ureteral jets (arrows) respectively on color Doppler evaluation of urinary bladder. These are normal findings and represent intravesical urine ejaculation due to pumping effects of calyceal peristalsis. Presence of strong jets argues against ureteral obstruction while their absence does not rule in obstruction. Bladder decompressed with Foley catheter: The empty bladder with functioning Foley catheter appears as a soft tissue wrapping around the anechoic fluid-filled Foley balloon (arrow), which appears like a cyst. Sometimes, a little bit of anechoic urine surrounding the balloon may be seen. Bladder wall abnormalities will not be appreciable in decompressed state. Malfunctioning Foley catheter: The image shows distended urinary bladder despite having a Foley balloon (arrow) in place indicative of an obstructed catheter, which can occur from a blood clot or other stricture Pelvic ascites mimicking urinary bladder: In this bladder area sonogram, the Foley balloon (arrow) appears to be located outside the bladder. However, the fluid collection anterior to the Foley is pelvic ascites and the Foley is in appropriate position. To confirm the diagnosis, we should perform a long axis scan which will show that this fluid collection is in continuity with the peritoneal cavity. This is another patient with ascites as evidenced by the free fluid throughout the abdomen. Bladder was decompressed and not visible in this sonogram. Uterus can be seen floating in the pelvic ascites and together with ovarian ligaments, it’s compared to a “TIE fighter” (‘Star Wars’ fictional Starfighter shown in the inset). Longitudinal exam of the bladder area demonstrates that this fluid is in continuum and anterior anechoic structure seen in transverse view is not urinary bladder. In this patient with ascites, anechoic ascites and bladder filled with urine (UB) can be seen as distinct entities both in longitudinal and transverse planes. Misplaced Foley catheter: In this image of long axis of the urinary bladder, the Foley balloon (arrow) is in the prostatic urethra resulting in urinary retention. Bladder with a small anechoic structure seen posteriorly, which likely represents a prominent ovarian follicle/cyst in a female patient. We know that it is not a blood vessel because there is no Doppler flow inside the structure (inset). Urinary bladder with internal echoes. If they persist after changing the angle of the ultrasound beam and adjusting the focal zone (to eliminate artifacts), correlate with cystitis/urinary tract infection. In this sonographic image of the urinary bladder, arrows point to diverticula (outpouchings of the bladder wall). They usually result from increased intravesical pressure from outlet obstruction, such as prostatic hyperplasia. Patient with chronic bladder outlet obstruction indicated by trabeculated bladder wall. Also note the significant post-void residual urine volume [Top panel is before voiding and the bottom panel after voiding]. Calculated bladder volume can be seen in the lower left corner of the images. Bladder stone seen as a hyperechoic structure (arrow) on grey scale image with acoustic shadowing (dotted area). A prominent twinkle artifact is seen on the color Doppler image. Another example of a bladder stone (yellow arrow) with acoustic shadowing (white arrow) and twinkle artefact (chevron). Echogenic debris can be seen in the bladder lumen, which likely indicates infection. Note that the debris related to infection usually moves with change in patient’s position while blood clots don’t. Enlarged prostate gland (arrows) compressing the urinary bladder. Note that the comprehensive evaluation of prostate for malignancy or other lesions should only be performed on transrectal scan. Partially filled urinary bladder demonstrating a focal echogenic area arising from the posterior wall. It was likely a blood clot because cystoscopy done 4 weeks later did not reveal any abnormality.
Common Ultrasound Scenarios in Nephrology
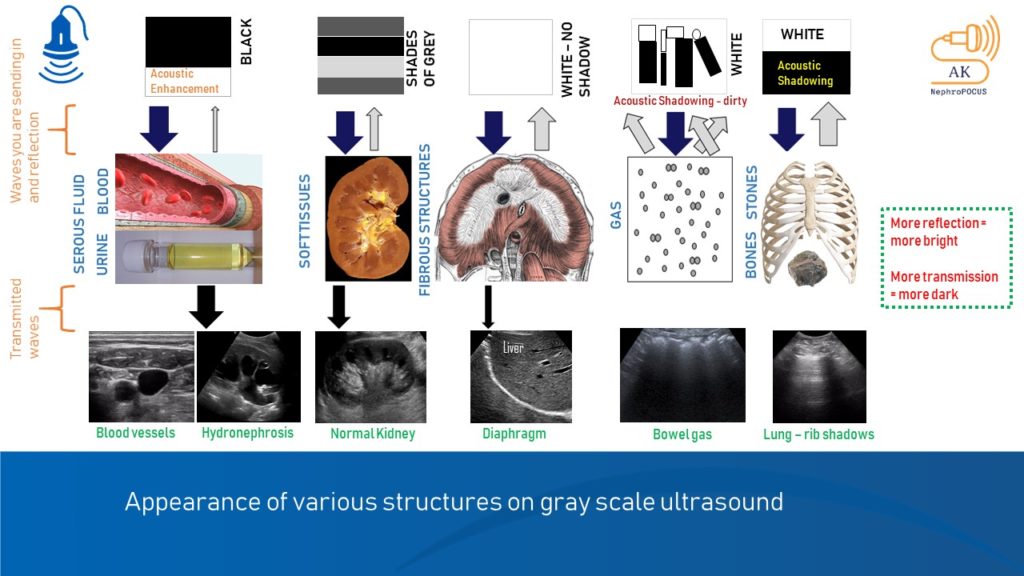
Common diagnostic point-of-care ultrasonography applications and clinical questions/pathologies pertinent to nephrology Kidney and urinary tract – common abnormalities part IKidney and urinary tract – common abnormalities part IIUltrasound findings in hypovolemiaUltrasound findings in hypervolemia Appearance of various structures on gray ultrasound