Exclusion of urinary tract obstruction is one of the most common indications for point of care ultrasonography (POCUS) performed by nephrologists and internists, as it is a potentially reversible cause of acute kidney injury. Though obstruction of urinary flow can occur at any site in the urinary tract, it is not uncommon to only look for hydronephrosis and ignore scanning the urinary bladder. Moreover, when a patient has an indwelling Foley catheter, we tend to ‘assume’ that the bladder is decompressed and absent urine output in such a patient is true anuria. However, ‘not passing’ urine cannot be equated to ‘not making’ urine until urinary catheter malfunction or malposition is excluded. Now, let’s figure out how to do this by going over some normal and abnormal sonographic images of the bladder area.
Figure 1: Normal urinary bladder
This is an illustration of a normal male pelvis accompanied by a normal urinary bladder sonogram in transverse plane. The urinary bladder appears as an anechoic fluid-filled structure (non infected urine is black on ultrasound) located in the mid pelvis. A full bladder is necessary to comprehensively evaluate the characteristics of its walls, contents and other pelvic organs. As structures closer to the probe are displayed on top of the ultrasound image, the top portion of this image represents the anterior aspect of the body and the bottom part corresponds to posterior

Figure 2: Decompressed urinary bladder with Foley catheter
Illustration of a normal female pelvis with a Foley catheter balloon (green dot) in the bladder accompanied by a sonographic image of decompressed bladder. The empty bladder with functioning Foley catheter appears as a soft tissue wrapping around the anechoic fluid-filled Foley balloon (arrow), which appears like a cyst. Sometimes, a little bit of anechoic urine surrounding the balloon may be seen.
Figure 3: Malfunctioning Foley catheter
The sonographic image demonstrates the transverse view of the bladder distended with urine despite having a Foley balloon in place (arrow). This is indicative of an obstructed catheter, which can occur from a blood clot or other stricture. A patient’s anuria can be treated by simply flushing the catheter. The green dot in the illustration corresponds to a Foley balloon in the distended bladder
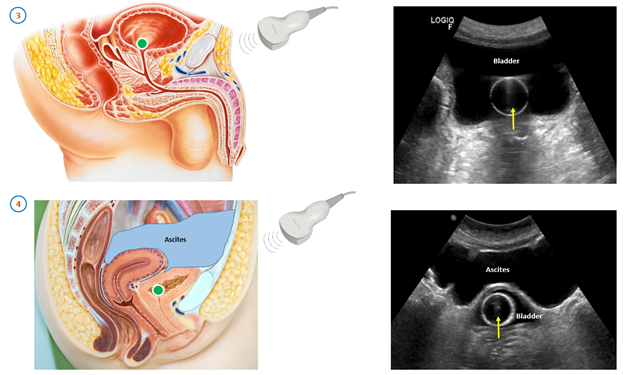
Figure 4: Pelvic ascites mimicking urinary bladder
In this bladder sonogram, the Foley balloon (arrow) appears to be located outside the bladder. However, the fluid collection anterior to the Foley is pelvic ascites and the Foley is in appropriate position as shown by the green dot in the illustration. Blood, serous fluid, and urine are all black on ultrasound. Note the margins of this ‘bladder-like’ structure are irregular which should make us suspect something isn’t right. To confirm the diagnosis, we should perform a long axis scan which will show that this fluid collection is in continuity with the peritoneal cavity. Moreover, a patient’s medical history should alert to the presence of pelvic ascites. That’s the whole point of POCUS – to know the patient well when we are performing the scan. It’s interesting to note that the bedside bladder scanning devices that are available in most hospitals these days can wrongly display ascitic fluid volume as bladder volume in this scenario.
Figure 5: Misplaced Foley in prostate
In this sonographic image of long axis of the urinary bladder, the Foley balloon (arrow) is in the prostatic urethra resulting in urinary retention. Note the anechoic urine filled bladder and prostate gland surrounding the Foley. This can be quite painful, but most of our ICU patients are sedated and cannot alert us to a complication. The illustration demonstrates the Foley balloon in the prostate represented by the green dot.

Figure 6: Misplaced Foley in vagina
This is the sonographic image of transverse view of the bladder showing Foley balloon (arrow) outside the bladder wall (posterior). Unlike our pelvic ascites case, this anechoic structure is regular in shape and is confirmed by long axis scan, which will demonstrate a contained fluid filled space not in continuity with the peritoneal cavity. The illustration of female pelvic anatomy shows that the vagina is posterior to the bladder and Foley catheter can be mistakenly placed in the vaginal canal (green dot), especially when the patient is sedated.
Take home point: You cannot exclude obstructive uropathy without scanning the bladder
Fun fact: Foley catheter was initially designed as a self-retaining balloon catheter to achieve hemostasis after cystoscopic prostatectomy by Dr. Frederic Foley in 1929.
Abhilash Koratala MD FASN (@NephroP)
NSMC Intern
University of Florida


Excellent description, illustrations, explanations. Very understandable. Kudos.