Welcome to the 33rd case of the Skeleton Key Group, a team of nephrologists from around the world who build a periodic education package for the Renal Fellow Network.
Author: Gilda Portalatin, MD @gildaportalatin
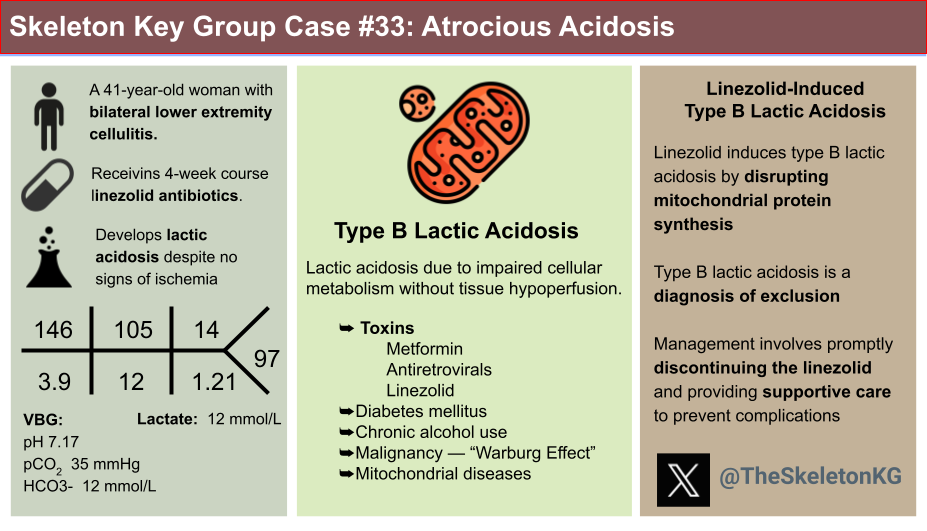
A. The Stem
A 41-year-old woman with stage I ovarian cancer complicated by lower extremity lymphedema presented to the emergency department with worsening leg swelling. In the month prior, she received multiple courses of antibiotics for bilateral lower extremity cellulitis but her symptoms worsened. Upon hospitalization, she underwent surgical debridement of necrotic tissue with skin grafting. Post-operatively, her vital signs were stable with fluid resuscitation and antibiotics. Wound cultures grew carbapenem-resistant Acinetobacter baumannii, E. Faecium, E. faecalis and mold for which she was started on a 4-week course of ampicillin-sulbactam, minocycline, linezolid, and voriconazole.
Despite normal vital signs postoperatively, she had worsening lethargy and lactic acidosis.
Vitals Post-Op
Temperature: 97.9 F
Blood pressure: 121/50 mm Hg (MAP 68)
HR: 97 bpm
RR: 22/min
SpO2: 99% on room air
Physical examination:
General: Lethargic
CNS: Awake, but confused
Cardiovascular: no murmurs, gallops or rubs
Respiratory: symmetric air entry, clear to auscultation bilaterally
Abdomen: Soft, non-tender, non-distended
Extremities: 3+ bilateral lower extremity edema with extensive dressing below the knee
Medications:
Ampicillin-sulbactam
Minocycline
Linezolid
Voriconazole
Apixaban for prior history of pulmonary embolism
Famotidine
Ferrous sulfate
Folic acid
Calcium carbonate-vitamin D
Hydromorphone
B. The Labs
Lactic acid upon initial presentation was 0.7 mmol/L, however it was up to 12.2 mmol/L at the time of consultation, hospital day 25.
C. The Work-Up
When working up any acid-base disturbance, obtaining a blood gas and using a systemic approach is key:
- Is the patient acidemic (pH<7.36) or alkalemic (pH >7.44)?
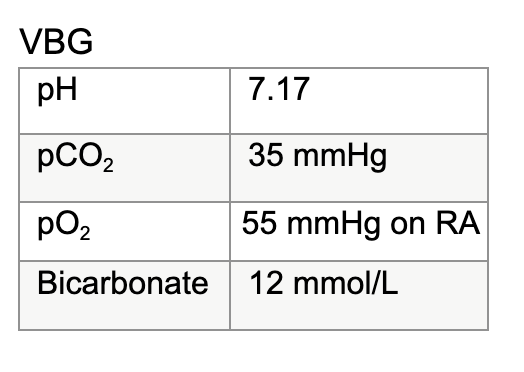
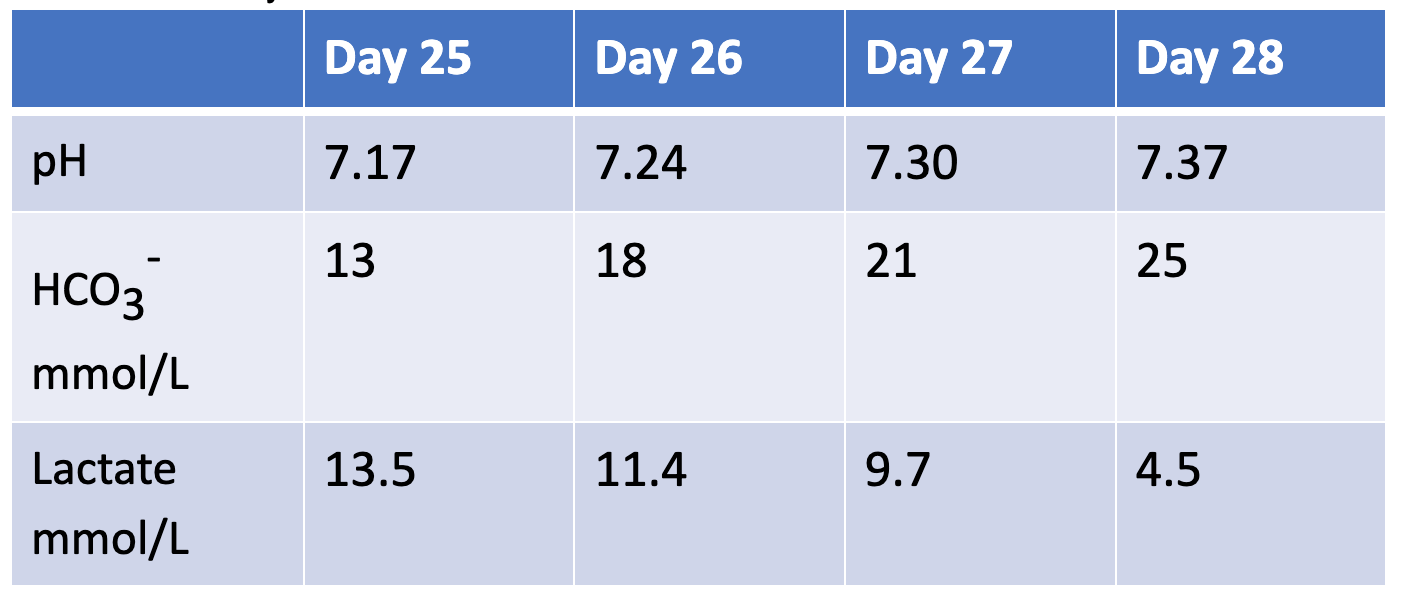
pH 7.16 indicating acidemia
- What is the primary disorder: Metabolic or Respiratory?
Bicarbonate of 12 mmol/L (low) demonstrating a metabolic acidosis
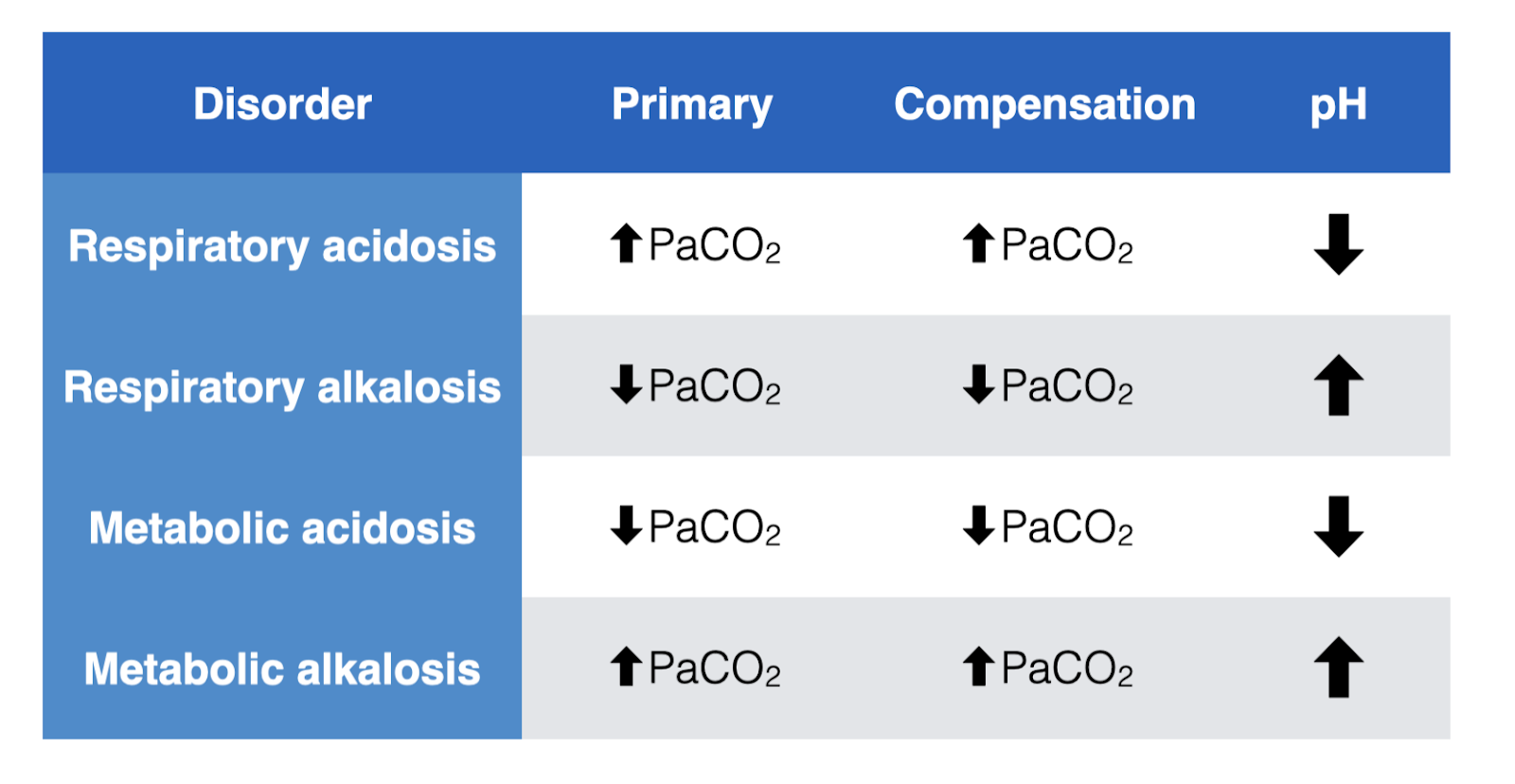
4. Is there adequate compensation?
Metabolic Acidosis: CO2= (1.5 x HCO–3) +8 ±2
- Using Winter’s formula: CO2= (1.5 x 12) +8 +/-2. Calculated CO2 falls between 24-28. The patient’s actual CO2 is 35 indicating a concomitant respiratory acidosis.
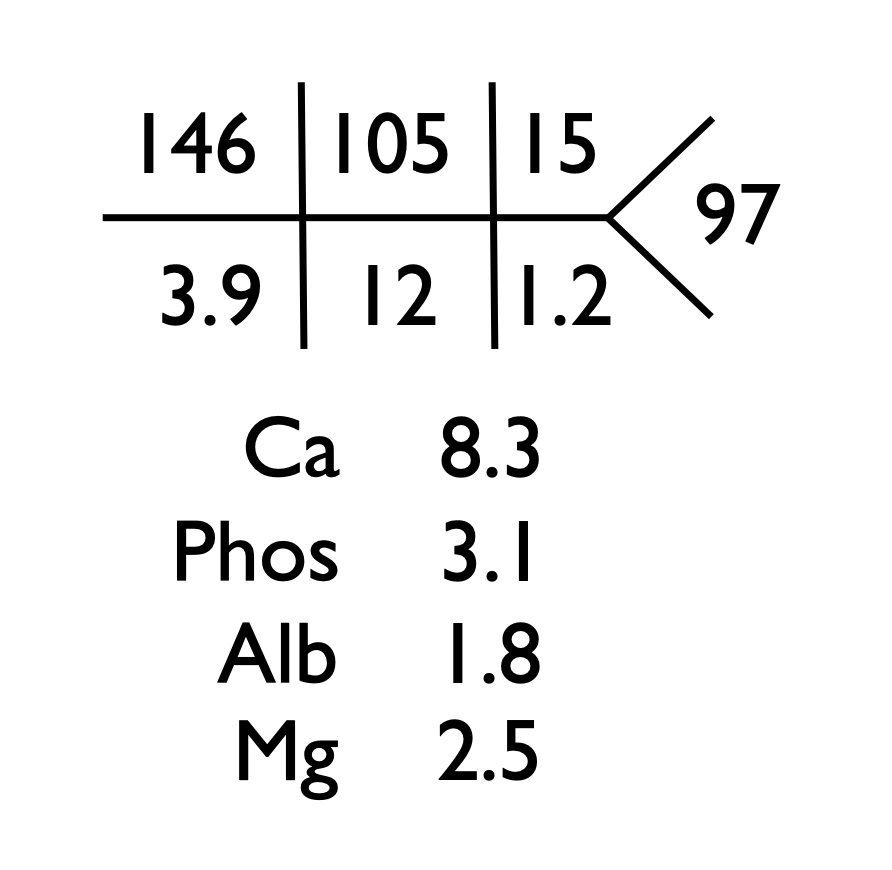
5. Is there an elevated anion gap?
AG= Na+ – [Cl + HCO3–]
- Anion gap= 146 – (105 + 12) = 29 (corrected for albumin 29.5)
6. Determine delta ratio to assess whether a mixed acid-base disorder present
(∆Anion Gap / ∆HCO3–):
- (29-12)/(24-12)= 1.4 indicating a pure high anion gap metabolic acidosis
Interpretation: Combined high-anion gap metabolic acidosis and respiratory acidosis.
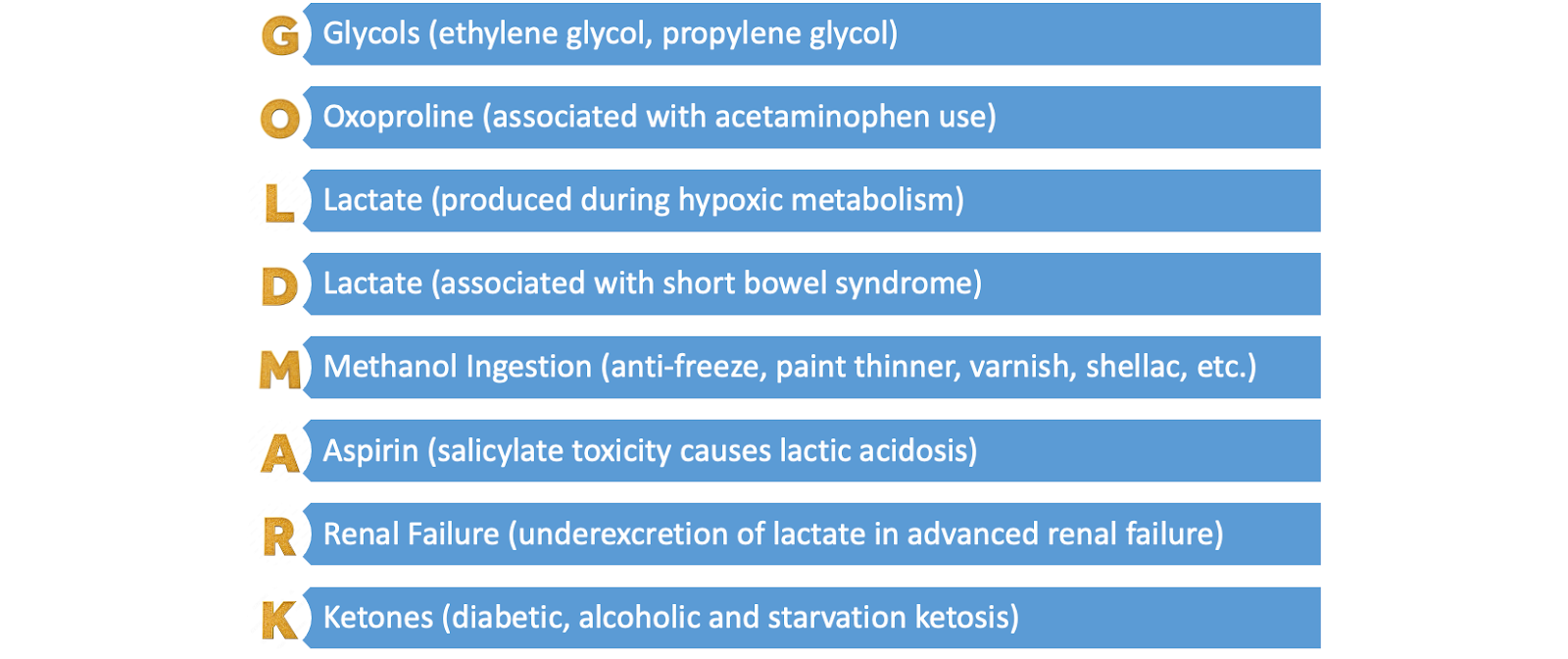
Don’t forget to work through the differential diagnosis of a high-anion gap metabolic acidosis using a mnemonic like GOLDMARK or MUDPILES—See our Skeleton Key Group Case #11 for a more in depth review! We exclude glycols, oxoproline, methanol, aspirin, renal failure, and ketoacidosis.
We concluded that the high-anion gap metabolic acidosis is likely due to the lactic acidemia, and the concomitant respiratory acidosis likely due to the respiratory depression from opioids post-operatively.
What’s causing the lactic acidosis?
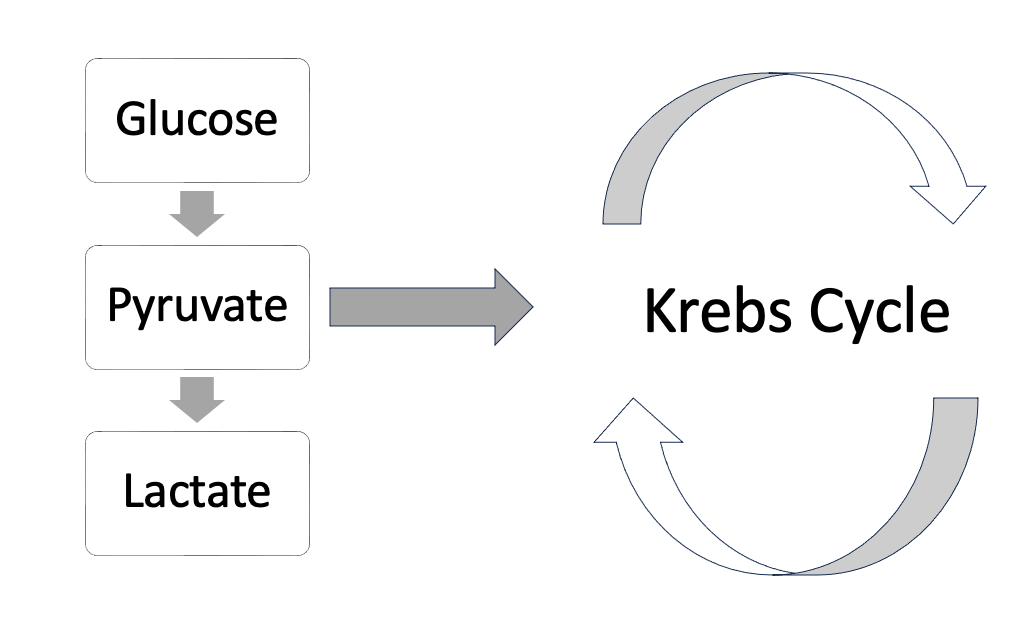
When we think about generating lactic acid, we start to reminisce about our biochemistry days, right? Remember that throughout multiple processes including glycolysis, gluconeogenesis and the Krebs cycle lactic acid is produced.
In order to better understand this, let’s breakdown the three types of lactic acidosis:
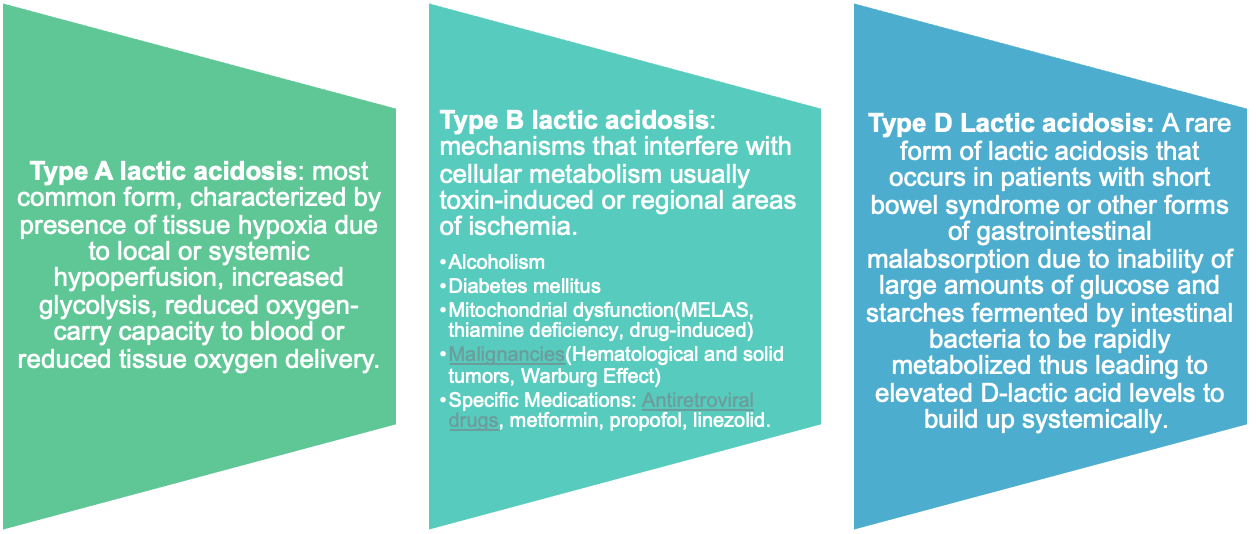
Type A is the most common form caused by local or systemic tissue hypoxia. It is unlikely because the patient has stable vital signs, adequate fluid resuscitation, and a postoperative CT was negative for signs of ischemia.
Type B is the lactic acidosis caused by disrupted cellular metabolism, and is usually a diagnosis of exclusion.
Type D is a rare form of lactic acidosis from short gut syndrome. Note: Standard assays for serum lactate measure L-Lactate and not D-Lactate!
Figuring out a Type B Lactic acidosis
DIFFERENTIAL DIAGNOSIS
➥ Toxins
Metformin
Antiretrovirals
Linezolid
➥Diabetes mellitus
➥Chronic alcohol use
➥Malignancy — “Warburg Effect”
➥Mitochondrial diseases
This patient does not have evidence of tissue hypoperfusion (Type A) or short gut syndrome (Type D) leaving us to consider the possibility of impaired cellular metabolism (Type B). Out of the potential causes of Type B lactic acidosis in this patient, we considered: malignancy-induced given her history of ovarian cancer, and toxin/medication-induced mitochondrial dysfunction. Cancers, especially hematologic (lymphoma, leukemia) and sometimes solid malignancies can generate lactic acidemia. One of the proposed mechanisms is the Warburg effect, where cancer cells convert glucose to lactate regardless of whether oxygen is present or not. However, our patient had undergone successful resection of her stage I ovarian cancer years ago and there was no evidence of recurrent disease on imaging. That leaves toxins/ medications. The most common causes are metformin, linezolid, and some antiretroviral medications. The patient was started on Linezolid with slow rise in lactic acid eventually peaking of 13 mmol/L at day 25.
D. Diagnosis
Suspected linezolid-induced type B lactic acidosis
This is a 41-year-old woman with a complex medical history including an infection of her lower extremity lymphedema requiring broad-spectrum antibiotics. Following debridement and skin grafting, she developed a high anion gap metabolic acidosis, despite normal vital signs and clinical stability and imaging studies negative for ischemia. With a lactic acid level peaking at 13.3 mmol/L and without other evidence of tissue hypoxia, we are thinking about Linezolid-induced type B lactic acidosis. This diagnosis was supported by the timeline correlating with Linezolid use, which can impair mitochondrial oxidative phosphorylation causing the production of lactic acid.
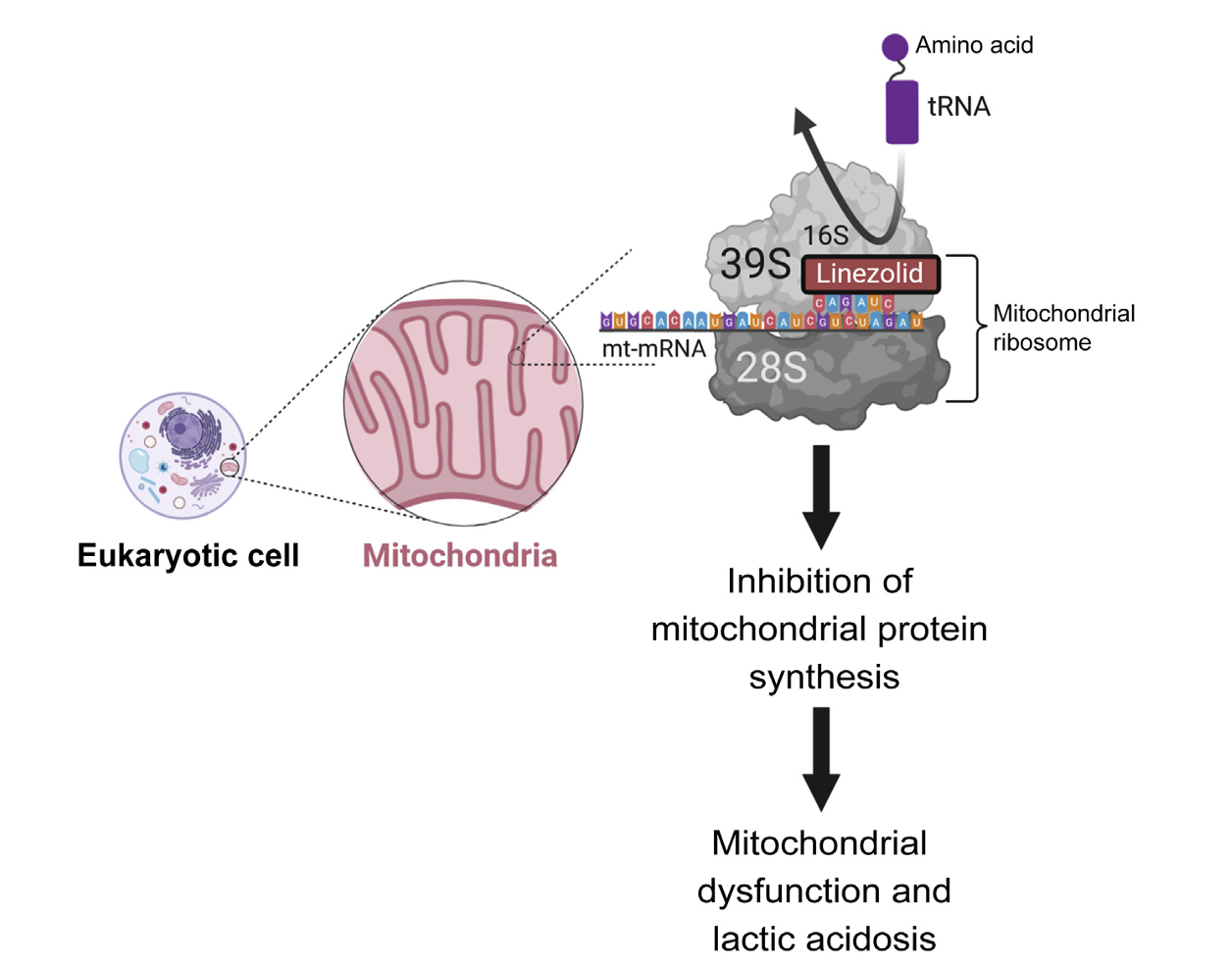
Image from Hindi et al.
Linezolid can impair mitochondrial protein synthesis in the respiratory chain complex thus limiting aerobic respiration and increasing lactate generation. Many reports have shown increased risk of developing severe acidosis with prolonged Linezolid use, however the exact timeframe still remains variable. Potential risk factors include increased risk with duration >6 weeks, advanced age, impaired kidney function and co-treatment with medications that impair linezolid clearance (e.g., omeprazole,amiodarone, amlodipine,rifampin).
Management
Linezolid should be discontinued immediately and the patient should receive supportive care.
Kidney replacement therapy should be used in severe cases to facilitate rapid clearance if the patient develops an indication for dialysis. Linezolid is 31% protein-bound, has a volume of distribution of about 30-50 L, and a half-life of approximately 5-7 hours, making it dialyzable if needed. However, lactic acidosis should not be the sole indication for renal replacement therapy unless other dialysis indications are present; we know that high-volume CRRT lactate removal is small in comparison to lactate generation. In this case, the patient received dialysis because of a pH <7.1 and lethargy/mental status changes. She received intermittent hemodialysis followed by continuous renal replacement therapy for three days. We refer to the EXTRIP workgroup guidelines for toxicology recommendations—although there are no specific recommendations for linezolid toxicity, the guidelines for metformin associated Type B lactic acidosis were helpful in this case.
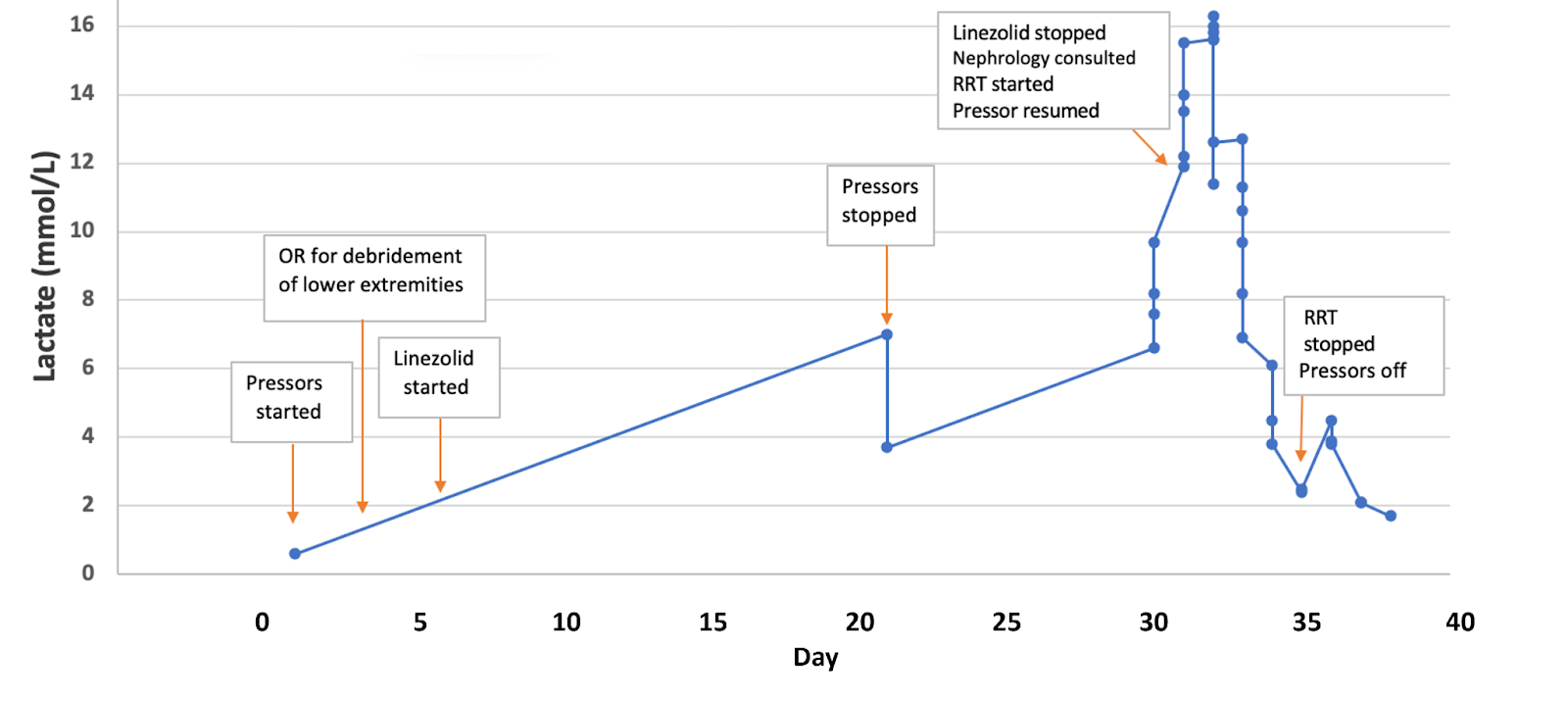
Follow-up
After cessation of linezolid and four days of kidney replacement therapy (one session of intermittent hemodialysis followed by three days of CRRT), the patient’s lactic acidosis resolved and her mental status improved. The patient was discharged to a long-term acute care facility.
E. Take-Home Points
- Linezolid can induce type B lactic acidosis by disrupting mitochondrial protein synthesis, which affects cellular metabolism
- Lactic acidosis is categorized into three types: Type A results from tissue hypoperfusion, Type B stems from impaired cellular metabolism (including drug-induced cases like linezolid), and Type D is associated with short gut syndrome
- Type B lactic acidosis is usually a diagnosis of exclusion necessitating a comprehensive evaluation to rule out other causes
- Management involves promptly discontinuing the linezolid and providing supportive care to prevent complications
Editors and Reviewers: Jefferson L Triozzi, Shweta Shah, Raad Chowdhury, Chi Chu, Joel Topf. Matthew A.Sparks, Margaret DeOliveira