Welcome to the 34th case of the Skeleton Key Group, a team of nephrologists from around the world who build educational content for the Renal Fellow Network.
Author: Nicole Wyatt
A. The Stem
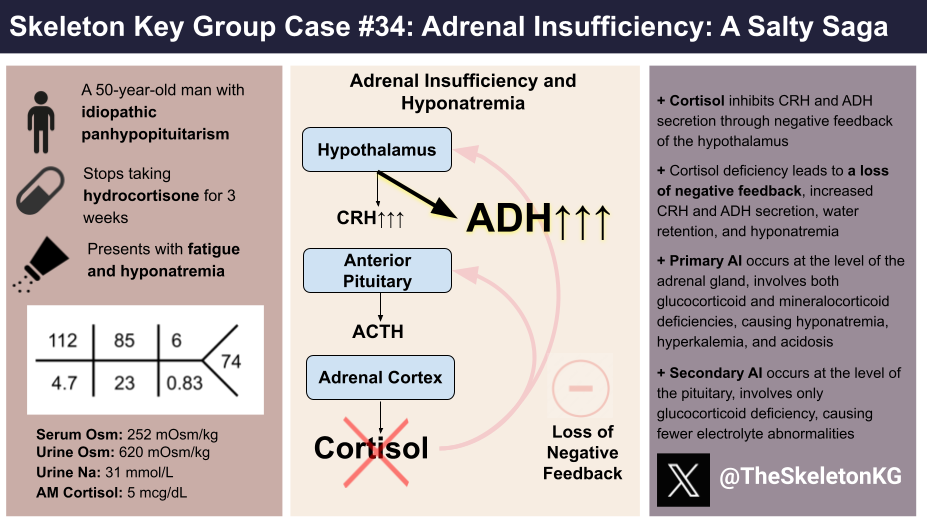
A 50-year-old man with idiopathic panhypopituitarism (adrenal insufficiency, hypothyroidism, hypogonadism) and substance use disorder presents to the emergency department for assistance in detoxing from methamphetamine. He was diagnosed with idiopathic panhypopituitarism 10 years ago after presenting with fatigue and weight loss. A work up showed low cortisol, ACTH, TSH, and LH with normal brain imaging. For the last 3 weeks, he did not take any prescribed medications (hydrocortisone 15 mg in AM and 10 mg in PM, levothyroxine, testosterone) due to his substance use disorder relapse. He reports fatigue, malaise, dizziness, and falls.
Vital Signs:
T: Afebrile
BP: 107/52 mm Hg
Pulse 83 BPM
Resp: 12 breaths per minute
SpO2 99% on room air
Weight 99.6 kg
Physical Exam:
General: well-nourished, not in any apparent distress
Neck: no jugular venous distention
Heart: normal rate and regular rhythm, no murmurs
Lungs: clear to auscultation bilaterally, not in respiratory distress
Abdomen: soft, non-tender, non-distended
Skin: no rashes in exposed areas, normal skin turgor
Extremities: no lower extremity edema
Neurological: normal strength and sensation.
Psychiatric: flat affect
B. The Labs
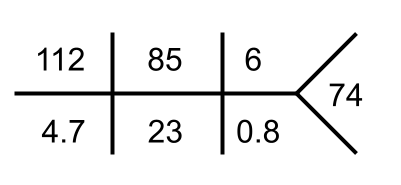
Serum Osmolality 252 mOsm/kg
Urine Na 31 mmol/L
Urine osmolality 620 mOsm/kg
Urine drug screen: + amphetamine, – ethanol
AM cortisol 5 mcg/dL
TSH 2.39 mIU/L, FT4 1.2 ng/dL
Uric acid 4.8 mg/dL
C. The Workup
Given our patient’s history of panhypopituitarism with medication non-adherence, his hyponatremia was thought to be due to central adrenal insufficiency. Let’s briefly review the structured assessment of hyponatremia before moving on (Check out some of our hyponatremia cases for a more detailed review).
Following confirmation of hypoosmolality (a serum osmolality <275 mOsm/kg), we evaluate urine osmolality to determine whether free water is retained due to the action of antidiuretic hormone (ADH). ADH is considered active if urine is not maximally dilute (i.e., a urine osm >100 mOsm/kg). Appropriate ADH action occurs in the setting of low effective arterial blood volume (EABV) due to volume depletion, heart failure, or cirrhosis. In these clinical scenarios, the renin-angiotensin-aldosterone system is activated resulting in low urine sodium (typically UNa <20 mEq/L). Inappropriate ADH action occurs when urine is concentrated despite normal or elevated EABV. This is the case with adrenal insufficiency, severe hypothyroidism, or syndrome of inappropriate ADH secretion (SIADH).
Differential Diagnosis: SIADH vs adrenal insufficiency
In this case, the patient has hypoosmolar hyponatremia (serum osmolality 252 mOsm/kg, serum Na 112 mEq/L) with a high urine osmolality reflecting the presence of ADH (Urine osmolality 620 mOsm/kg). He also has a euvolemic physical exam and urine sodium > 20 meq/L suggesting inappropriate ADH activity. It can be difficult to distinguish between adrenal insufficiency and SIADH since they both can have this pattern! Correct diagnosis is imperative as adrenal insufficiency responds to glucocorticoid administration while SIADH is treated with fluid restriction, removing inciting factors, and at times solute administration with or without loop diuretics. Vasopressor receptor antagonists may also be used in special circumstances. Therefore, it is important to have a low threshold to order a morning serum cortisol to distinguish adrenal insufficiency from SIADH.
D. The Diagnosis
The diagnosis of adrenal insufficiency can be made based on a low serum cortisol level (consider diagnosis in <18 mcg/dL, diagnosis likely in <3 mcg/dL), which is checked in the morning within 3 hours of waking. An ACTH level is also acquired to differentiate primary vs. secondary/tertiary, with high/high normal ACTH in primary adrenal insufficiency and low/low normal in central adrenal insufficiency. In cases that are indeterminate based on the ACTH level (upper half normal), plasma aldosterone and plasma renin may be checked for confirmation because low aldosterone and high renin are consistent with primary adrenal insufficiency.
Adrenal Insufficiency: A Brief Review
The hypothalamo-pituitary-adrenal axis includes corticotropin-releasing hormone (CRH) from the hypothalamus → adrenocorticotropic hormone (ACTH) from the pituitary gland→ cortisol from the adrenal gland. Aldosterone is also produced by the adrenal gland however it is dependent on the renin-angiotensin system.
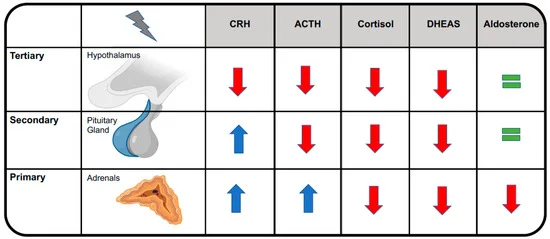
Image by Coluzzi et al.
Primary adrenal insufficiency is due to adrenal gland dysfunction, including autoimmune adrenalitis, infections, metastatic cancer, adrenal hemorrhage, withdrawal of chronic steroids and medications (including ketoconazole, fluconazole, etomidate). When the dysfunction occurs at the level of the adrenal gland, both cortisol and aldosterone are deficient.
Central adrenal insufficiency, results from dysfunction at the level of the pituitary gland (secondary adrenal insufficiency) or the hypothalamus (tertiary adrenal sufficiency). Etiologies for central adrenal insufficiency include mass lesions, infiltrative lesions, radiation, infections, medications, and many more. Cortisol and other hormones produced by the pituitary, are affected in central adrenal insufficiency, but the ability of the adrenal gland to excrete mineralocorticoids remains intact.
Pathophysiology of hyponatremia in adrenal insufficiency
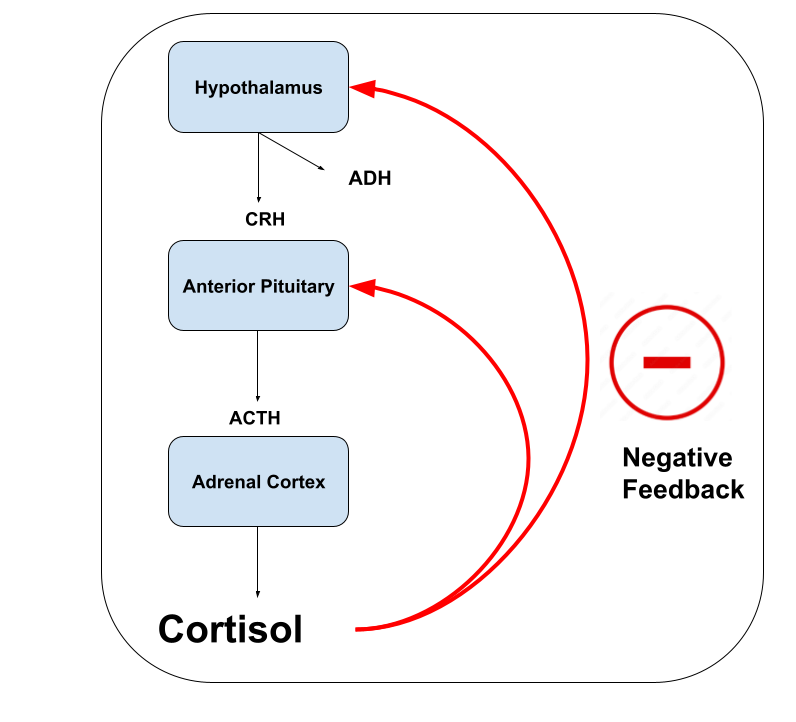
Normal Cortisol-ADH Negative Feedback:
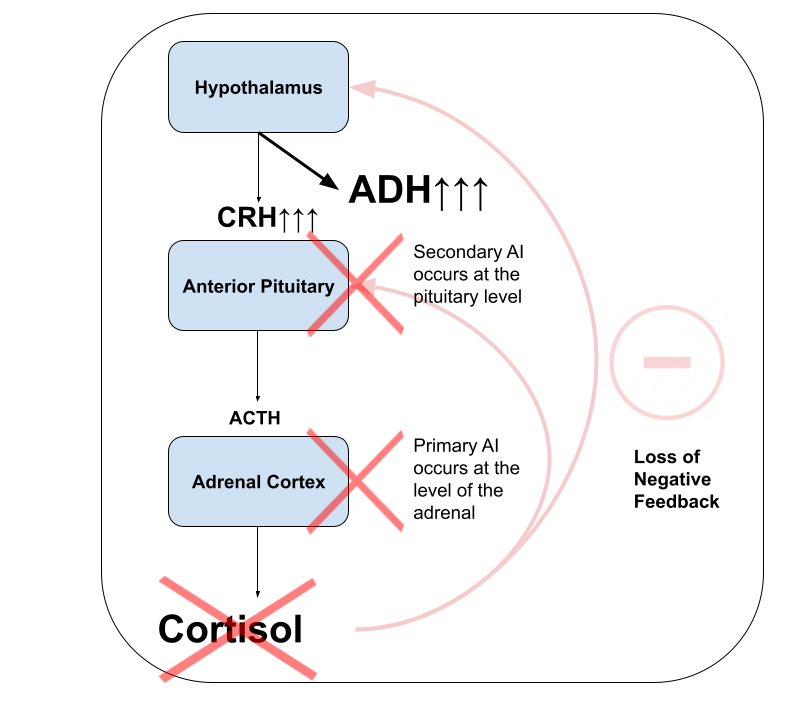
Loss of Cortisol-ADH Negative Feedback in Adrenal Insufficiency:
The pathophysiology of hyponatremia in adrenal insufficiency involves two major mechanisms:
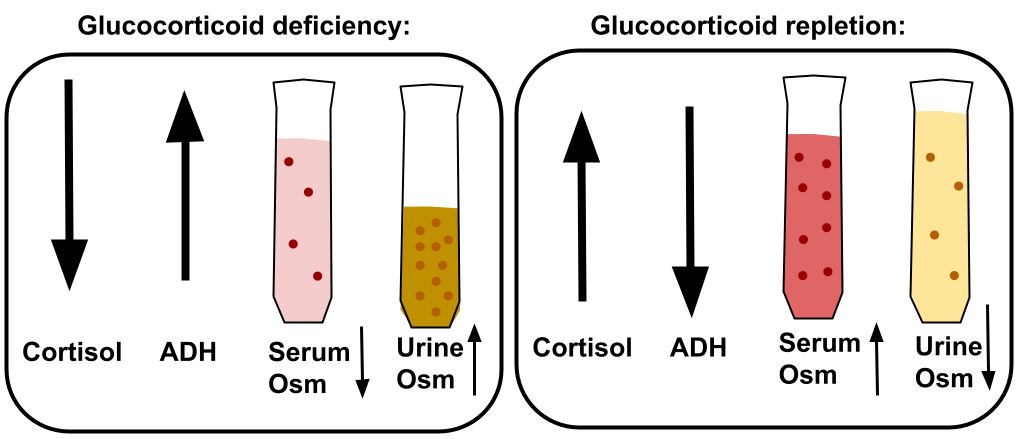
1) hypersecretion of ADH due to cortisol deficiency (both primary and secondary adrenal insufficiency). Normally, cortisol inhibits CRH and ADH secretion through negative feedback on the hypothalamus. This means a cortisol deficiency leads to increased CRH and ADH secretion by the hypothalamus. Excess ADH leads to hyponatremia due to retention of water (E.g., “inappropriate” ADH release). Though the full mechanism is not fully understood, the reason for this negative feedback is to moderate activation of the hypothalamic-pituitary-adrenal axis in response to stressful stimuli.
2) mineralocorticoid deficiency (only primary adrenal insufficiency). Lack of aldosterone causes sodium wasting in the distal nephron and volume depletion, which also leads to hypovolemic ADH release (E.g., “appropriate” ADH release). In addition to sodium wasting, loss of aldosterone leads to the hyperkalemia and normal anion gap metabolic acidosis seen in primary adrenal insufficiency. The presence of these other electrolyte and acid-base abnormalities are clues to a primary adrenal insufficiency.
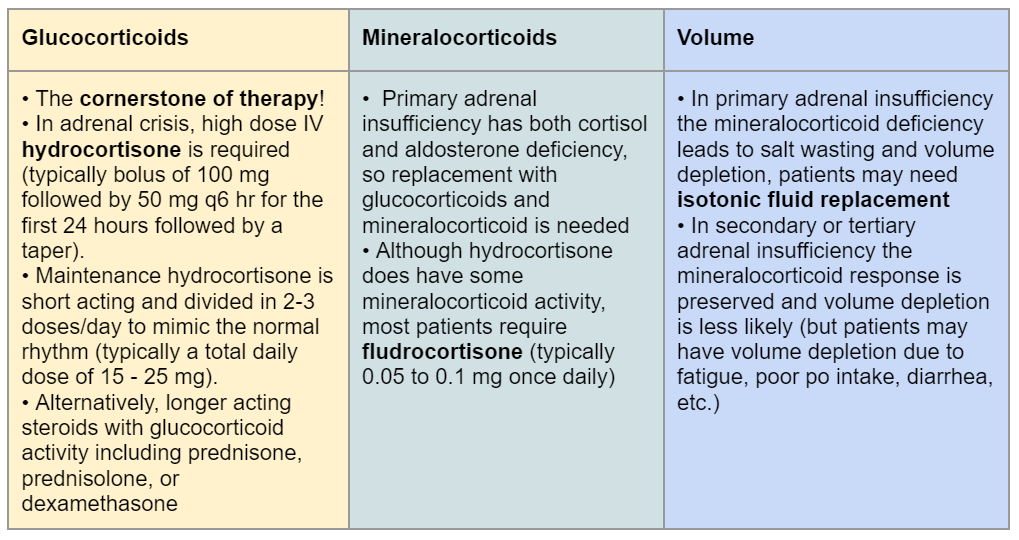
Management
The cornerstone of management is steroids. Remember that primary adrenal insufficiency (adrenal gland dysfunction) causes both glucocorticoid and mineralocorticoid deficiency and requires both glucocorticoid and mineralocorticoid replacement. Secondary or tertiary adrenal insufficiency (pituitary or hypothalamic dysfunction, respectively) only requires glucocorticoid replacement because the adrenal gland can still produce aldosterone.
Patients sometimes require volume replacement, particularly primary adrenal insufficiency which causes significant kidney sodium wasting and volume depletion due to the lack of aldosterone. Regardless of the method used to correct the hyponatremia, correction of sodium should be limited to no faster than 8 mEq/L/day to minimize the risk of osmotic demyelination syndrome (ODS). Patients with adrenal insufficiency are at high risk of overcorrection due to suppression of ADH after glucocorticoid administration and the subsequent water diuresis. These patients should be monitored closely and are good candidates for a DDAVP clamp depending on the level of hyponatremia and other factors present.
Case summary
Let’s put the “salty saga” together:
This case is a great example of hyponatremia due to adrenal insufficiency. Glucocorticoids were started on day 1 but for unclear reasons he stopped receiving them on days 2-3. Observe how the sodium and urine osmolality studies change with and without glucocorticoids:
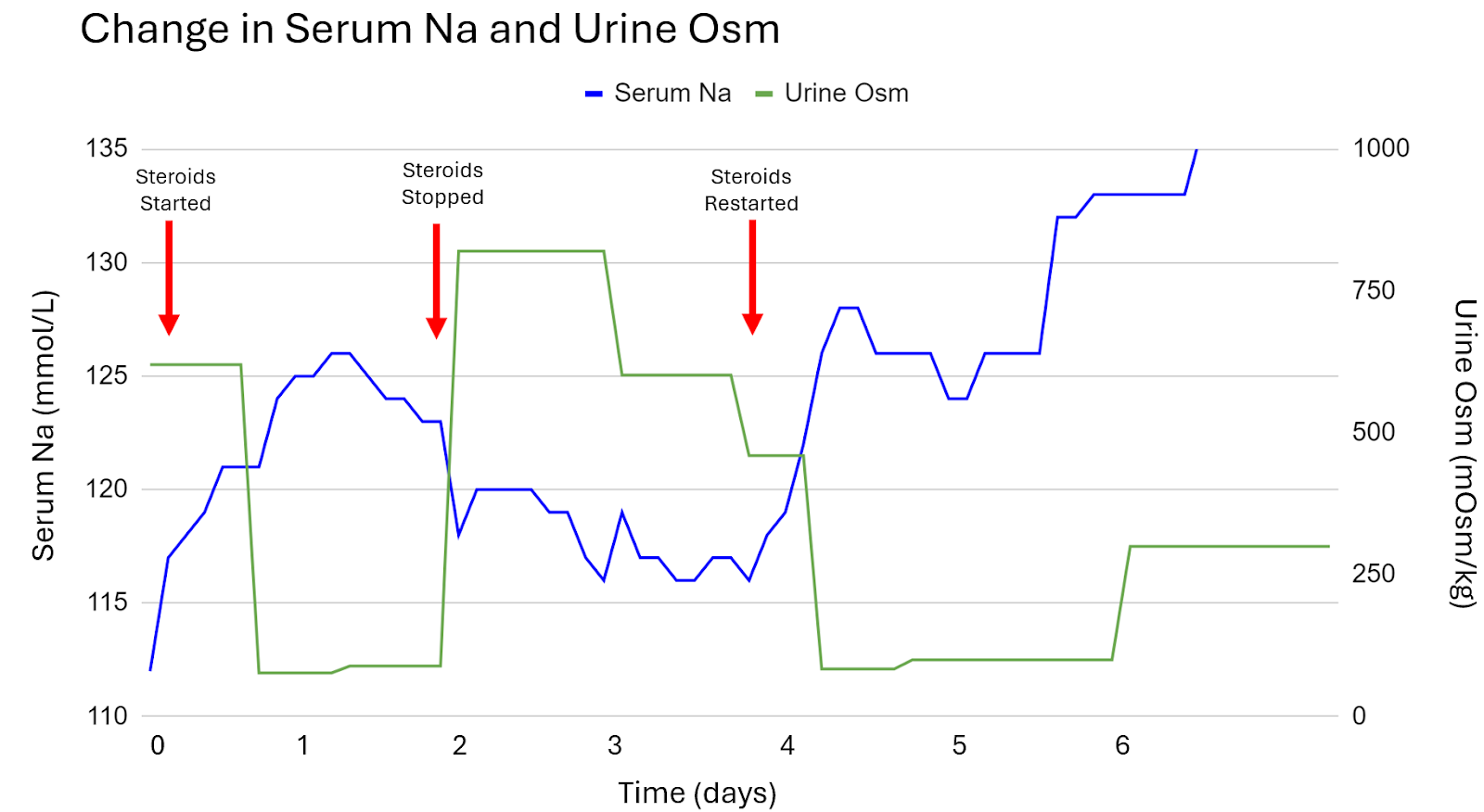
| Day | Serum Sodium (mEq/L) | Urine Osm (mOsm/kg) | Events |
| Day 0 (Baseline) | 112 | 620 | Diagnosis: Hyponatremia due to adrenal insufficiency |
| Day 1 | 112→121 →126 | 620→89 | Steroids started: IV methylprednisolone 40 mg to start then hydrocortisone 50 mg QID for maintenance. |
| Day 2 | 126→118 | 89→820 | Nephrology consulted for overcorrection of sodium, started a DDAVP clamp and D5W. |
| Day 3 | 120→116 | 602→460 | Due to unclear reasons, the patient did not receive steroids on day 3 which caused his sodium to decline to 116 despite discontinuation of DDAVP clamp and D5W. |
| Day 4 | 118→128→126 | 460→84 | Steroids resumed: hydrocortisone 50 mg QID, received a D5W bolus to mitigate overcorrection. |
| Day 5 | 126→132 | 84—>102 | Steroids continued, sodium correcting. |
| Day 6 | 132→138 | Steroids continued, normonatremia. |
Ultimately, the patient continued maintenance medications and was discharged with a stable serum sodium.
E. Take Home Points:
- Both primary and secondary adrenal insufficiency can cause hypoosmolar hyponatremia and should be considered in the diagnosis of ADH-dependent hyponatremia, one with appropriate ADH, and one with inappropriate ADH.
- Cortisol normally inhibits ADH secretion. A cortisol deficiency leads to excess ADH secretion causing water retention and hyponatremia.
- The treatment of choice for primary and secondary adrenal insufficiency is hydrocortisone. Primary adrenal insufficiency may also require treatment with fludrocortisone to correct sodium loss, excrete potassium, and restore circulating volume.
- Patients with adrenal insufficiency are at risk for overcorrection of hyponatremia as glucocorticoid therapy promptly resolves the excess of ADH secretion, leading to a brisk water diuresis with rapid rise in serum sodium.
Editors:
Jefferson L Triozzi, Payal Gaggar, Joel Topf, Chi Chu, Trey Richardson, Matthew A. Sparks, Margaret A. DeOliveira