 Recently we had a patient who, despite good adherence to dietary restrictions and 4 hour dialysis runs, had a high pre-dialysis potassium and an inadequate URR. She had an AVF with a history of multiple central stenoses and we suspected a recurrence. Her venous pressure wasn’t very high but we asked the nurses to check for recirculation.
Recently we had a patient who, despite good adherence to dietary restrictions and 4 hour dialysis runs, had a high pre-dialysis potassium and an inadequate URR. She had an AVF with a history of multiple central stenoses and we suspected a recurrence. Her venous pressure wasn’t very high but we asked the nurses to check for recirculation. R = ([P – A] / [P – V]) x 100
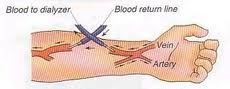
where P= BUN periphery, A= BUN arterial line, V= BUN venous line and R= % recirculation
The issue that arises is from where to take the peripheral sample. Previously, the sample was taken from the contralateral arm. The problem with this is that mixing of blood returning from the AVF with returning systemic venous blood lowers the BUN in the heart relative to the periphery, leading to an overestimation of the BUN of the blood entering the AVF and therefore an overestimation of the percentage recirculation. This problem could be fixed by taking the sample from an artery but this is obviously impractical. Nowadays, most units use a protocol that involves stopping or slowing the blood flow through the dialyzer temporarily in order to take a sample from the arterial line which closely approximates the BUN of blood entering the AVF.
In our unit, the protocol involves taking arterial and venous samples, slowing the blood flow to 100mls/min for 30 seconds, withdrawing 10mls of blood and discarding it and then drawing the ‘peripheral’ sample from the arterial port. Although this technique probably underestimates recirculation slightly, it is sufficient to make the diagnosis. Recirculation of >15% is considered significant.
In this case, the % recirculation approached 50% and the patient had a fistulogram which showed a stenosis in the venous limb of the AVF and her clearances improved following angioplasty.


If you need info on backflow testing los angeles. Then the internet has excellent resources.
Great post. Used it at the bedside today for teaching with housestaff.
If P and A are equal, the equation will read:
R = 0 / P – V = 0
By definition, if P = A, there is no recirculation so R should = 0
if BUN from P and A are same, numerartor will be zero. how will one be able calculate R?
I would have used the Transonics monitor ,and performed an ABF test And a Recirculation test to verify recirculation…MUCH EASIER AND FASTER