Being a parent is probably one of the most desirable and difficult tasks in life.
While ESRD is associated with a high rate of infertility related to hormonal changes and anovulation, most patients undergoing renal transplantation resume menstrual cycles and fertility in approximately 6 months!
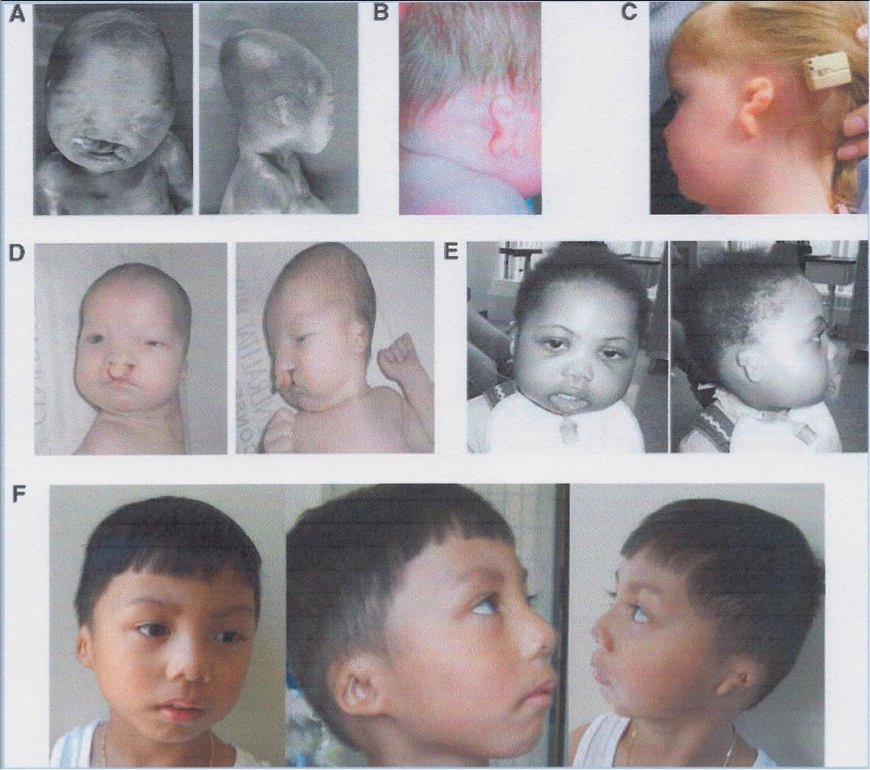
Contraception is critical post-transplant due to potential teratogenicity of MMF (1st trimester pregnancy loss, facial and limb deformities as can be seeing on the figure). It is essential to plan ahead of time for patients interested in getting pregnant once renal allograft function is stable for at least 6 months.
Conversion from MMF to AZA must be done at least 2 months prior to conception.
Best timing of pregnancy is unclear though waiting at least 1 year after transplant is generally recommended.
Most common immunosuppressive regimens are tacrolimus or cyclosporine with AZA +/- prednisone.
The incidence of birth defects in recent cohort was similar to the proportion in the general population of 3–5%. Few cases of successful in vitro fertilization (IVF) have been reported as well.
Approximately 30% of patients also suffer deterioration of kidney function after pregnancy. Overall perinatal mortality at 5.8% was almost six times higher among babies born to transplant recipients than among the general population.
Specific management:
– If pregnancy occurs on MMF, stop medication right away and performed careful counseling to couple (about 40% risk of miscarriage and 30% risk of malformations)
– Convert MMF to AZA. A dose of 500mg BID of Cellcept equals approximately 200mg AZA, though variability of metabolism and weight has to be taking into account. After conversion, monitor LFTs and WBC. No need to overlap drugs during conversion.
– Monitor CNI levels since they may vary during pregnancy (Monthly Levels – 1st and 2nd trimester and weekly levels on third trimester)
– Start calcium and vitamin D for bone protection in addition to folate-containing multivitamin
– Check TSH on each trimester
– Stress dose steroids recommended during maternal distress and in labor (e.g. hydrocortisone 50mg during active labor).
– There is paucity of data regarding breastfeeding and consequences of immunosuppressive drugs in the fetus.
Next time you see a young female transplant recipient, please don’t forget to discuss about methods of contraception in addition to their usual immunosuppressive drugs!! Being aware of risks and planning ahead of time can prevent devastating consequences to the new parents…

nice information you provied and you finding The best IVF Centre in Ludhianawhere you can get effective treatment.
I want to know how safe is it to switch from MMF to AZA in tacrolimus based immunosuppression therapy in renal transplant recipient?
Relative to your comment that MMF seems to be deleterious only during embriogenesis, should a women get off Cellcept (and if yes for how long?) if she is not considering pregnancy, but is planning to harvest her eggs for IVF and embryo implantation into a surrogate gestational carrier?
Thanks Paul for the comment. No data but MMF seems to be deleterious only during embriogenesis, therefore it does not seem to affect the ovule or sperm quality. Though there have been some suggestions of decreased sperms with certain immunosuppressive therapy (e.g. rapamycin). So it is important to keep that in mind…
Nice post. I've always wondered about male patients on MMF who want to father a child. Any evidence of risk? No guidelines to come off MMF as far as I know.