Tazeen Rizvi, MD
Advocate Christ Medical Center
Oak Lawn, IL

Epidemiology: A Peripherally inserted Central Catheter (PICC) is a 50 to 60 cm long single, double, or triple lumen catheter, which is placed in a peripheral arm vein and terminates in the thorax. They can be used for anywhere from weeks to months, making them attractive when long-term intravenous access is needed. Due to their use in the inpatient and outpatient settings, PICC lines are extremely common.
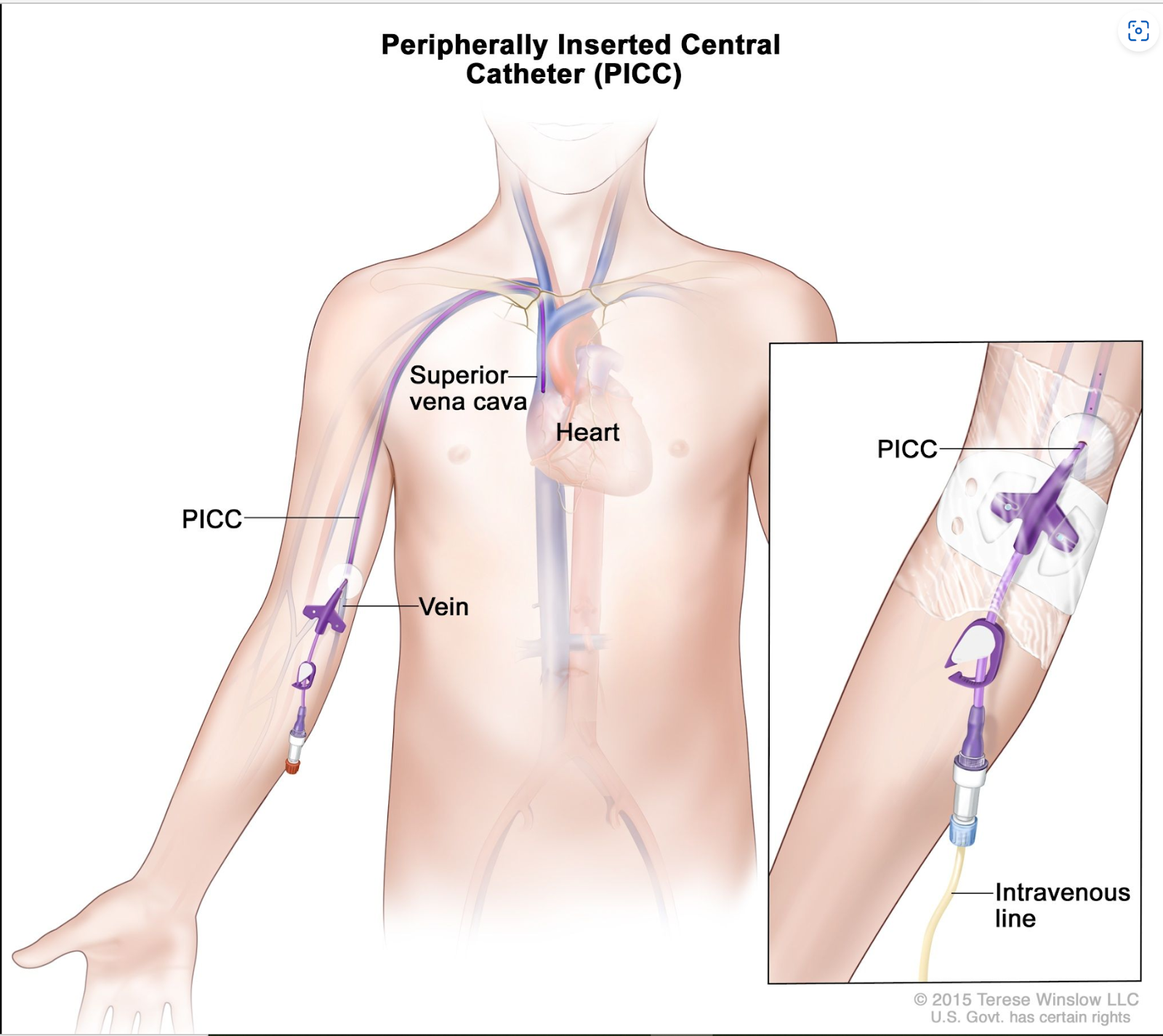
Usually, a PICC can be inserted through the basilic, brachial, medial cubital or cephalic veins, eventually terminating into the SVC (superior vena cava). The right basilic vein is the most preferred site of insertion, due to its larger size and straighter trajectory to the SVC. Additionally, the right basilic vein is more desirable because of fewer valves, better hemodilution capabilities and a shallower angle of insertion compared to other veins.
Indications: PICC lines may be considered in individuals who need long term IV medications, total parenteral nutrition, continuous administrations of medications, administration of medications not compatible with peripheral veins, rapid infusions, blood product administration, or in patients that have limited peripheral access. Additionally, patients with coagulation disorders, like thrombocytopenia, may benefit from PICCs so as to limit phlebotomy sticks and the potential for pain, bruising, or swelling that would make repeated blood draws more challenging.
Relative Contraindications: Patients with kidney failure undergoing arterial-venous (AV) access planning need to preserve veins as possible conduits for dialysis in the future. Placement of a PICC may lead to stenosis and eventual sclerosis of critical venous structures. Additionally, use of crutches (as they may place pressure on the vein), active bacteremia, burns, trauma, skin infections, radiation, or a history of venous thrombosis at insertion site may make placement of a PICC technically difficult or increase risk of complications.
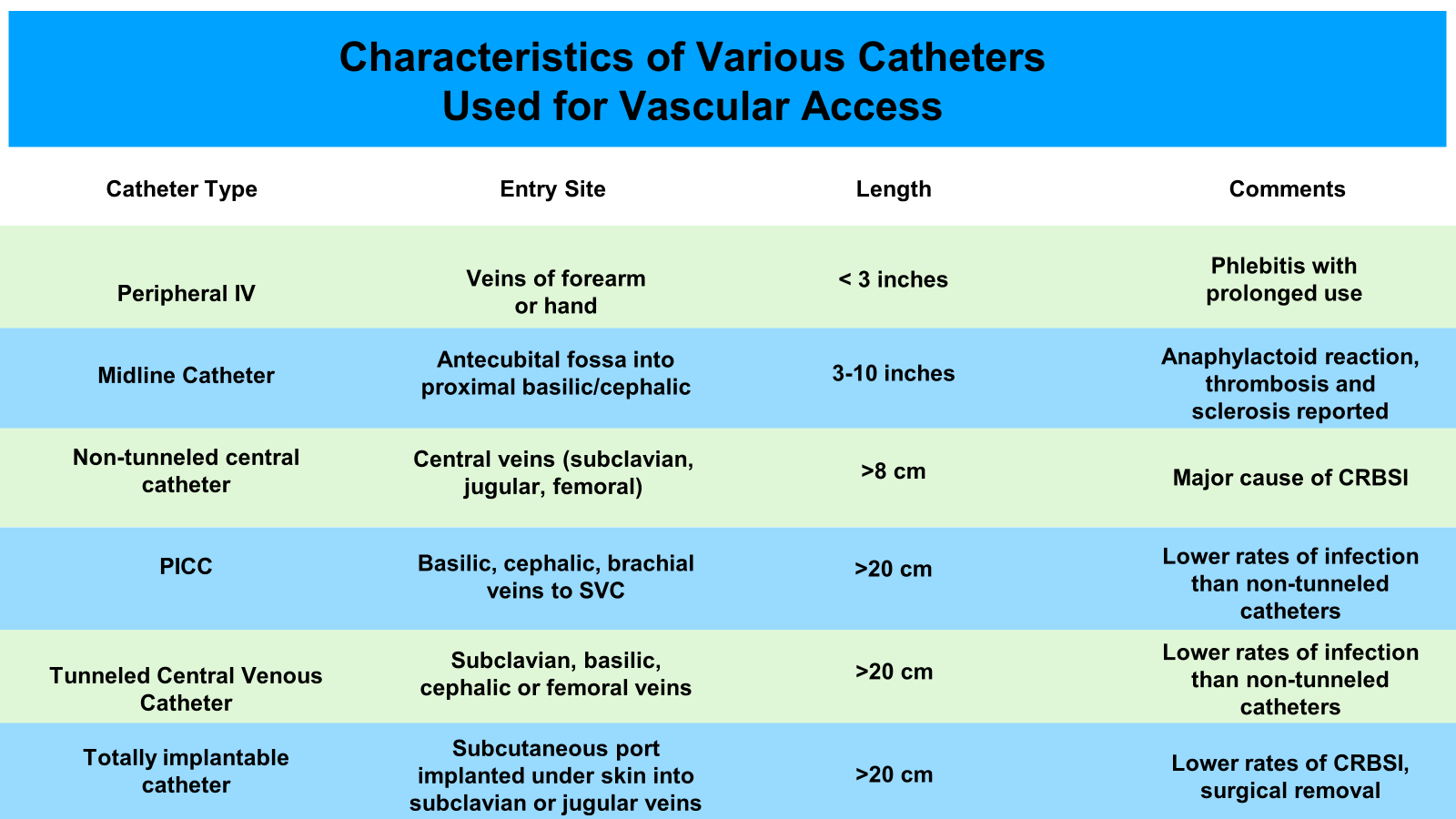
Alternative Access: Introduced in the 1950s, midlines are unique vascular access devices. Like PICC lines, midlines are also inserted in the peripheral (basilic, cephalic, brachial) veins, however, unlike their counterparts they terminate in the peripheral vasculature. As a result, the risk of metastatic bloodstream infections (i.e endocarditis, discitis) are potentially lower with midlines. However, in terms of venous structure disruption, midline catheters pose similar risks of venous sclerosis/thrombosis and therefore the same guidelines as PICCs should be applied.
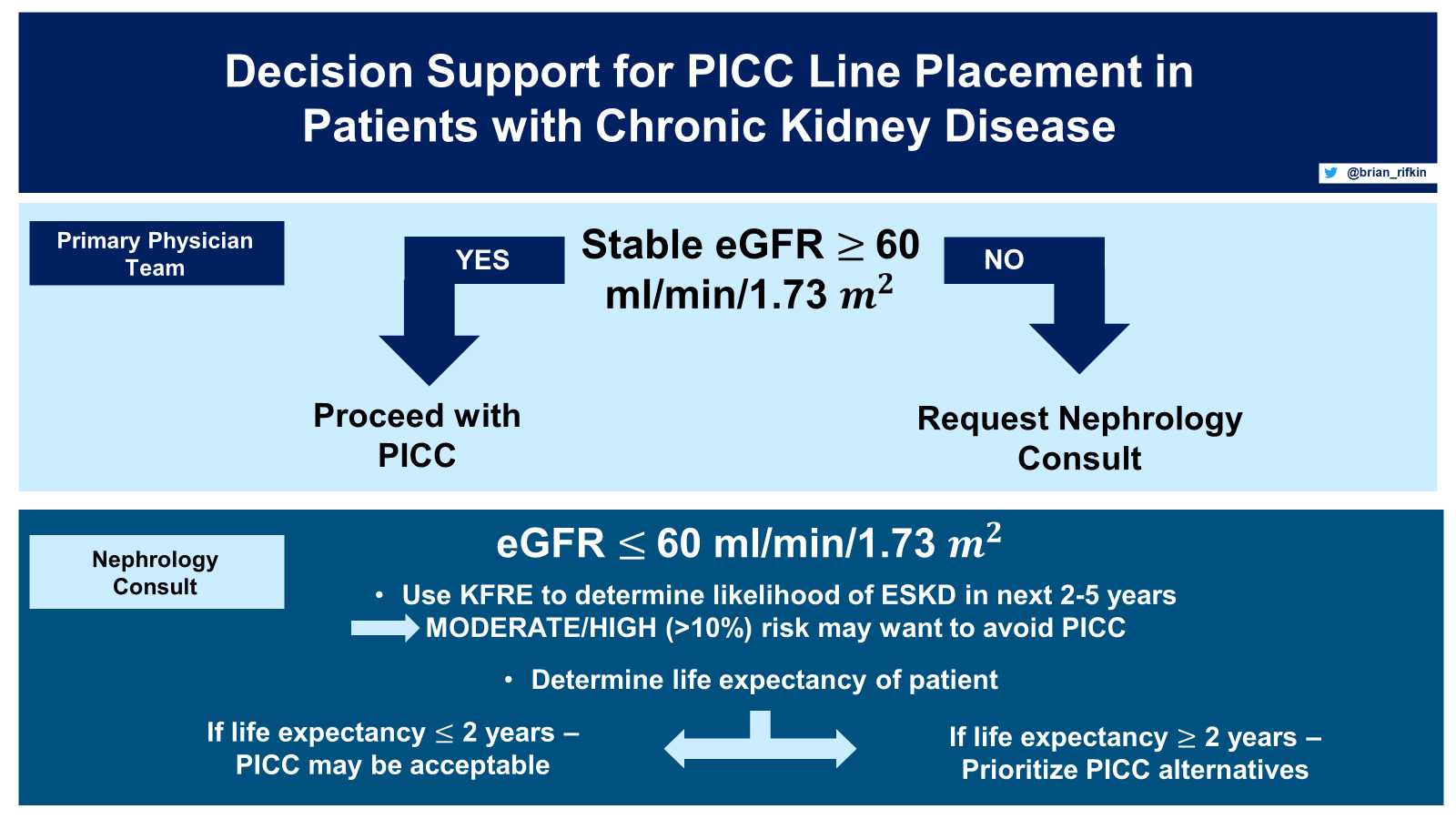
When to involve Nephrology: Despite the usefulness of midlines and PICC lines, nephrologists are often posed with the question of whether they are acceptable in CKD stage 3-5 patients. The reason behind this query is the possibility of a patient requiring an AV access once the patient has progressed to ESKD. PICCs and midlines tend to be inserted into the Basilic vein, an ideal site for creation of an AV access. Typically, post PICC/midline placement patients can develop vein sclerosis, stenosis or even thrombosis. A retrospective analysis performed by Allen et al, reported a 38% incidence of deep venous thrombosis with PICCs. Additionally, the incidence varied by placement site, with rates of 10% in brachial vein, 14% in basilic vein and 57% in cephalic vein. Lack of viable veins creates barriers to the successful creation of an AV access, which in turn may make patients dependent on dialysis catheters. Dialysis catheters, independent of their duration of use, carry a much higher risk of infection, dysfunction and patient mortality than AV fistulas or grafts. According to Bharvi P Oza et al, when choosing whether to place a PICC line in CKD patients, it is essential to estimate the risk of CKD progression to ESKD. Hence, the first step is to use an equation such as the Kidney Failure Risk Equation (KFRE) to help predict the risk for developing kidney failure. The KFRE uses the patient’s urine albumin-creatinine ratio (ACR), sex, age and eGFR to project the probability of requiring dialysis in the next 2 to 5 years. The KFRE was originally created using 2 independent Canadian cohorts of CKD stage 3-5 patients from 2001 to 2008. The equation has shown similar observed and predicted risk for patients in North American; however, it overestimated the risk in non-North American populations, hence calibration may be necessary for this group when using the KFRE. Regardless of eGFR, if life expectancy is less than 2 years, then proceeding with PICC may be appropriate. On the other hand, if life expectancy is greater than 2.5 years, and the possibility of hemodialysis exists, then other alternative CVC access should be considered.
What can be used alternatively: PICC line insertion poses a potential risk to successful AV access creation. A Quality Initiative by the American Society of Anesthesiology in 2020 completed consensus guidelines focusing on CVC use. These guidelines did not specifically address the needs of CKD or ESKD patients. Similarly, the KDOQI 2019 vascular access guidelines only addressed the use and complications of dialysis catheters and not other forms of CVCs. There are currently no society consensus statements on the use of CVC catheters in CKD/ESKD, but it is generally accepted to:
- Obtain consultations to determine if oral medications offer a reasonable therapeutic alternative to IV medications. This difference in administration route, especially with antibiotics, can remove the need for CVCs altogether.
- Use peripheral IVs in patients with eGFR < 60 mL/min/1.73 m2 depending upon the proposed duration of therapy. Avoiding large gauge IVs in the antecubital veins when possible, especially if AV access creation is imminent.
- Use small-bore, central venous tunneled catheters (i.e. Hickman catheter) if the expected duration of IV medication administration exceeds 5 days, or if a central vein is required for medication administration. This should be placed in the internal or external jugular vein. The subclavian vein should be avoided as it is a smaller diameter vessel, due to compression by the clavicle, and has increased risk of vascular injury and thrombosis.
- If there are no feasible alternatives to a PICC line in patients likely to need AV access placement in the future, a short-term, small-diameter PICC may be acceptable, preferentially placed in the deep brachial vein.
- Patients with ESKD should preferentially receive IV antibiotics with dialysis as appropriate, based upon cultures and sensitivities, to avoid use of CVCs.
Despite the recommendations regarding using tunneled small-bore CVCs instead of PICC lines when AV access creation is probable, it is unclear if this is the ideal solution. Insertion of tunneled small-bore CVCs in the recommended locations requires more resources (fluoroscopy/ultrasound guidance) and expertise. Alternatively, PICC line insertion is often accomplished at the bedside without imaging. However, these steps do lead to preservation of the basilic and cephalic veins, hence minimizing risk of AV access failure due to a lack of viable veins.
Reviewed by: Brian Rifkin, MD, Edgar V. Lerma, MD, Matthew A. Sparks, MD