Mohammad Ahsan Sohail, MD
Nephrology & Hypertension Fellow PGY-5
Department of Kidney Medicine, Cleveland Clinic
Tushar Vachharajani, MD, FASN, FACP
Chair, Department of Medicine, John D. Dingell Department of VA Medical Center
Vice Chair, Department of Medicine, Wayne State University School of Medicine
Acknowledgements:This post is part of a collaboration between The Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. For more information about the ASDIN mission or membership, click here. Special thanks to the ASDIN Fellows Education Committee for their support on this project.
Introduction
Common sites to create an arteriovenous fistula (AVF) are at the wrist between the radial artery and cephalic vein (radio-cephalic AVF), and at the elbow between the brachial artery and cephalic vein (brachiocephalic AVF). An arteriovenous graft (AVG) involves the placement of interposing material, usually made of expanded polytetrafluoroethylene (ePTFE), to connect an artery and a vein, typically in the arm or leg. Although permanent AV access with either an AVF or AVG is preferred, a tunneled dialysis catheter may be required for initiation of hemodialysis or in patients with failed AV access. The right internal jugular (IJ) vein is the preferred site for insertion of hemodialysis catheters as it provides a direct path into the superior vena cava (SVC). The left IJ can be used, however, the trajectory requires the catheter to make two right-angle bends and an anteroposterior bend over the pulmonary arch before reaching the SVC (Fig 1). Subclavian vein catheter placement is avoided due to the narrowing of the subclavian vein as it passes under the clavicle, which can lead to central vein stenosis and compromise construction of upper extremity AV hemodialysis access. The development of central vein stenosis, secondary to (non-dialysis related) central venous catheters and cardiac implantable electronic devices, may also hamper the creation of conventional forms of hemodialysis access. The lower extremity veins are less frequently utilized, but may be accessed in patients with occluded upper extremity or central veins. Thus, conservation of central and peripheral veins is crucial for vascular access creation. Consequently, patients with exhausted vasculature require innovative approaches to create hemodialysis accesses at unconventional sites.
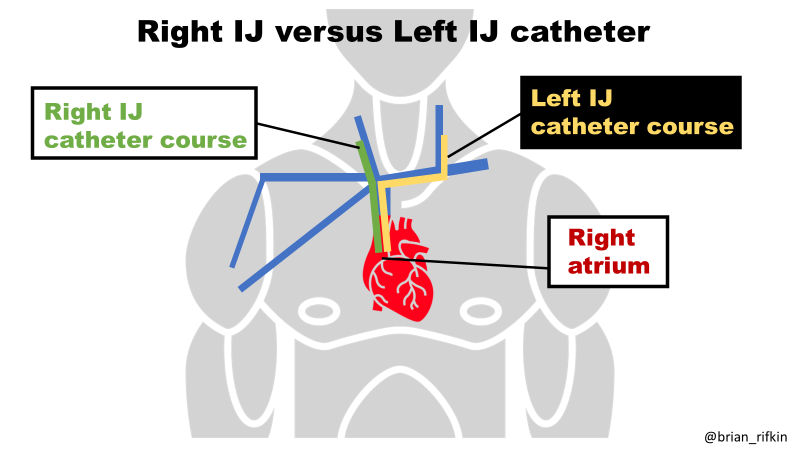
Figure 1. Course of internal jugular venous catheters
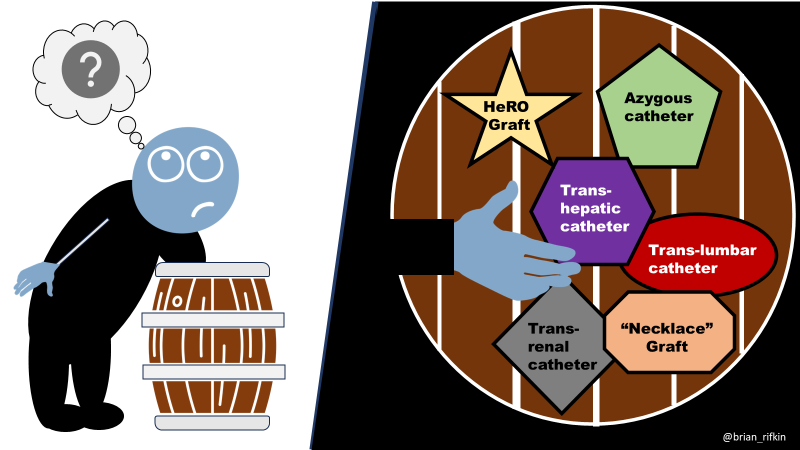
Unconventional Sites for Hemodialysis Catheter Placement
Trans-Lumbar Catheters
The trans-lumbar approach utilizes percutaneous cannulation of the infra-renal IVC just lateral to the lumbar vertebrae (Fig 2). It was first described in 1971 by Mirete et al, and represents one of several unconventional approaches for hemodialysis catheter insertion in patients with concomitant SVC and IVC occlusion. Although the rate of infectious complications with trans-lumbar dialysis catheters (2.6/1000 catheter days) is similar to that of traditional hemodialysis catheters, trans-lumbar catheters exhibit higher rates of dysfunction and poor long-term access survival. For instance, according to a retrospective analysis from one center involving 39 trans-lumbar catheters, the cumulative trans-lumbar catheter patency rate at 1 and 3 years was 73.2% and 27.9% respectively. In the IJ catheter cohort from the same center had primary patency rates of 77.8% at 1 year and 44.0% at 3 years. Similarly, in another study involving 62 patients with bilateral central vein occlusion with loss of upper limb hemodialysis access, the 3- and 12- month patency rates for trans-lumbar catheters were 75.4% and 28% respectively, which were worse than those for tunneled femoral catheters (88% at 3 months and 50% at 12 months).
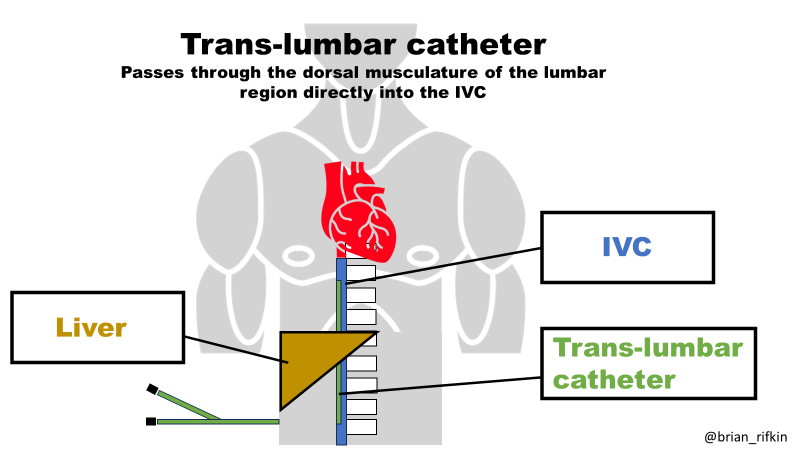
Figure 2. Intravascular position of trans-lumbar catheter
Trans-Hepatic Catheters
Trans-hepatic catheterization was initially described by Po, et al in 1994. The technique involves percutaneous cannulation of the right, middle or left hepatic vein (Fig 3). According to a large prospective study involving 296 patients who underwent trans-hepatic catheter insertion, technical success was achieved in all cases with the tip of the catheter placed in the right atrium in 80% of the patients. Reported complications included catheter migration, catheter related bloodstream infections (CR-BSI) and thrombosis (0.14, 0.15 and 0.18 per 100 catheter-days respectively) with a mean duration of catheter function of 280 days. Compared with traditional hemodialysis vascular access sites, trans-hepatic catheters are associated with a higher rate of placement-related complications such as arterial injury and hematomas. However, in contrast to trans-lumbar catheters, trans-hepatic catheters can be used in patients with occluded lower IVCs, and are associated with a lower risk of complications including hemorrhage and migration.
Figure 3. Intravascular placement of trans-hepatic catheter. Tip may be in IVC or right atrium depending on the level of thrombosis.
Trans-Renal Catheters
Trans-renal catheters represent another last-resort vascular access option in patients in whom conventional and trans-lumbar access have been exhausted (Fig 4). Percutaneous trans-renal access was first reported in 2002 in a patient with an occluded infra-renal IVC, a small-caliber supra-renal IVC and a pre-existing infected trans-lumbar catheter. According to the largest reported multicenter retrospective cohort study (6 trans-renal insertions and 4 replacement procedures), the mean primary patency duration was 107.3 ± 70.9 days. The procedure is associated with a significant risk for arterial injury and operators should be skilled in renal arteriography and embolization.
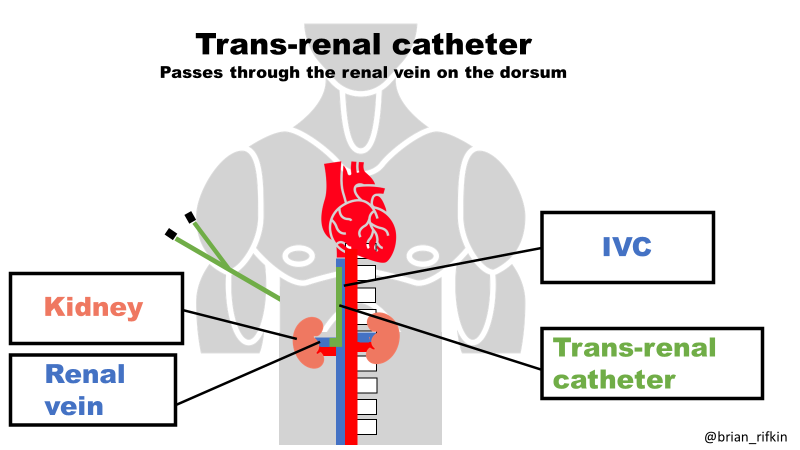
Figure 4. Intravascular placement of trans-renal catheter. Very rarely used in clinical practice.
Azygos Vein Catheters
Azygos vein catheterization, via a percutaneous trans-lumbar ultrasound guided approach, was reported initially in 2000 for administration of total parenteral nutrition and antibiotics. Although the inadvertent cannulation of the azygos system has been described, one report demonstrated that an azygos vein dialysis catheter was successfully utilized for 6 months (Fig 5). Another case report described the successful trans-lumbar placement of a hemodialysis catheter into the azygos vein in a patient with thrombosis of all conventional vascular sites, including the IVC. Unfortunately, even though azygos vein cannulation represents another viable option in the setting of exhausted vascular access, it is associated with a higher rate of CR-BSIs and catheter dysfunction, compared with other dialysis catheter sites, necessitating frequent exchanges.
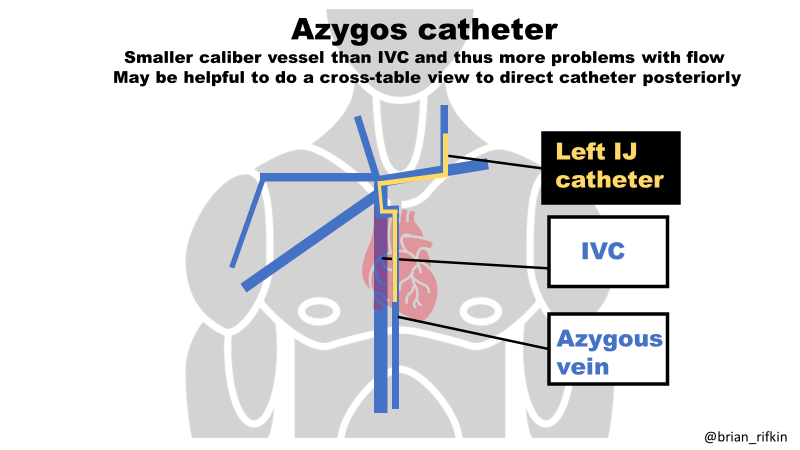
Figure 5. Azygos vein placement via IJ. Catheters may be placed in the azygos from the IJ or translumbar position.
Intra-Atrial Catheters
The open surgical creation of an intra-atrial hemodialysis access is another example of a high-risk, extreme salvage procedure which is potentially life-saving in patients with venous capital exhaustion. Intra-arterial catheters carry a much higher risk of air embolization, which can cause peripheral tissue necrosis. In addition, the higher pressures of an arterial catheter may lead to frequent alarms from the dialysis machine. Retrospective studies involving 34 patients who underwent intra-atrial dialysis catheter placement reported median survival rates of only 19-41 months, and catheter dislodgement was a common complication. A meta-analysis of all 51 cases of intra-atrial catheter insertion from the literature also demonstrated a poor median survival time of 25 months. Nonetheless, intra-atrial access placement (where available) should still be considered a lifesaving technique in patients with severe comorbid conditions and terminally exhausted venous access.
Arteriovenous Access Options for Patients with Exhausted Vasculature
Uncommon Locations for AV Grafts/Fistulas
Patients who have undergone multiple access procedures often experience central venous stenosis and occlusion. Axillary artery-based arteriovenous grafts can be utilized in patients with ipsilateral central vein stenosis. For instance, a subclavian or brachiocephalic occlusion can be bypassed if a chest wall ‘necklace’ graft is created between an axillary artery and the contralateral axillary vein. One study involving 35 patients who underwent axillary-axillary AVG operations reported primary patency of 88% at 6 months and secondary patency of 54% at 48 months, comparable to upper extremity ePTFE grafts. Given these grafts have also demonstrated a lower infection risk when compared to AV thigh grafts, they should potentially be preferred over AV grafts involving the lower extremities.
On the other hand, patients with a total SVC occlusion may also have completely exhausted upper extremity vasculature, and end up requiring AV access placement in the lower extremities instead (Fig 6). Examples of AV accesses created in the lower extremities include thigh grafts (between the common or superficial femoral artery and the femoral or saphenous vein), as well as fistulas from the saphenous vein to the femoral artery and very rarely, in the lower leg from the saphenous vein to the posterior tibial artery. Even though thigh AV grafts offer respectable secondary survival rates (1-,2- and 5 year survival rates of 62%, 54% and 38% respectively) and infection-free survival rates (1-, 2- and 5 year survival rates of 79%, 73% and 61% respectively), they are associated with a much higher risk of infection when compared to upper extremity grafts (11.1% for thigh graft vs. 5.2% for upper extremity graft; P=0.07). Lastly, in patients with concomitant complete SVC and IVC occlusion, an AV graft connecting the femoral artery to the right atrium may be regarded as a last-ditch attempt at long-term dialysis access prior to considering insertion of trans-lumbar or trans-hepatic hemodialysis catheters.
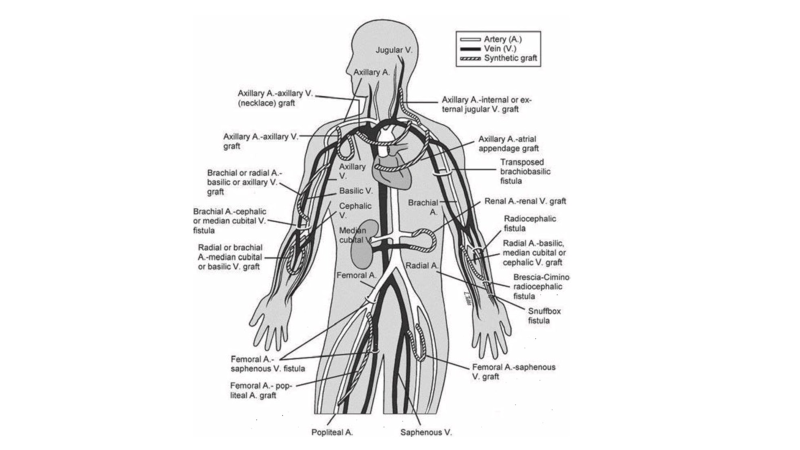
Figure 6. Typical and unusual locations for AVG placement Paulson WD, Ram SJ, Zibari GB. Vascular access: anatomy, examination, management. Semin Nephrol. 2002 May;22(3):183-94
Hemodialysis Reliable Outflow (HeRO) Grafts
The HeRO graft is an arterio-venous hybrid access device that has three components: a 6 mm ePTFE graft component, a single-lumen outflow catheter component, and a titanium connector. The graft component is typically placed in a subcutaneous tunnel in the upper arm and anastomosed to the brachial artery, whilst the catheter or ‘venous outflow’ component enters the central venous circulation via the internal jugular vein with the distal tip of the catheter positioned in the right atrium.
The HeRO device has been specifically proposed as an alternative access for those catheter-dependent patients with exhausted upper extremity vasculature and central venous stenosis in whom the next step would normally involve placement of a thigh AVG (Fig 7). The initial prospective study investigating HeRO device outcomes involving 36 patients who were poor candidates for AVF/AVG, and demonstrated similar function and patency compared with conventional AV graft outcomes, along with a significantly lower rate of bacteremia compared to the tunneled dialysis catheter literature control (0.7 vs. 2.3 per 1000 days). A systematic review, involving 409 HeRO grafts from 8 studies, demonstrated primary and secondary patency rates of 21.9% and 59.4% respectively, along with low rates of bacteremia (0.13-0.7 events per 1000 days) and steal syndrome (6.3%).
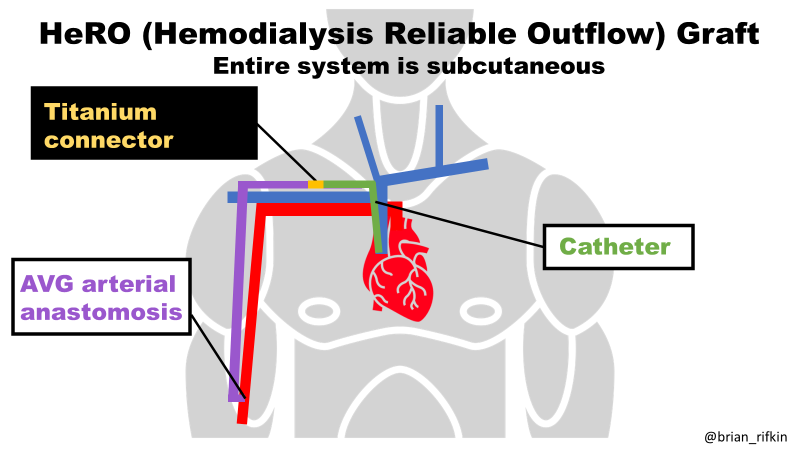
Figure 7. HeRO graft placement with area in upper arm used for cannulation, similar to AVG.
Conclusion
Arteriovenous access creation, in patients requiring hemodialysis, can be challenging as venous targets are exhausted. Creativity by surgeons and interventionalists is necessary to create viable accesses for patients who may have limited options. Robust randomized clinical trials are needed to identify the most suitable patient population for novel devices and vascular targets for complex access-challenged dialysis patients. Until kidney transplants become universally available, new technologies and strategies are needed to create and maintain dialysis accesses.
Reviewed by: Brian Rifkin, Sam Kant, Margaret DeOliveira