Welcome to the 32nd case of the Skeleton Key Group, a team of nephrologists from around the world who build a monthly education package for the Renal Fellow Network.
Authors: Nolan Interial, James Alstott
A. The Stem
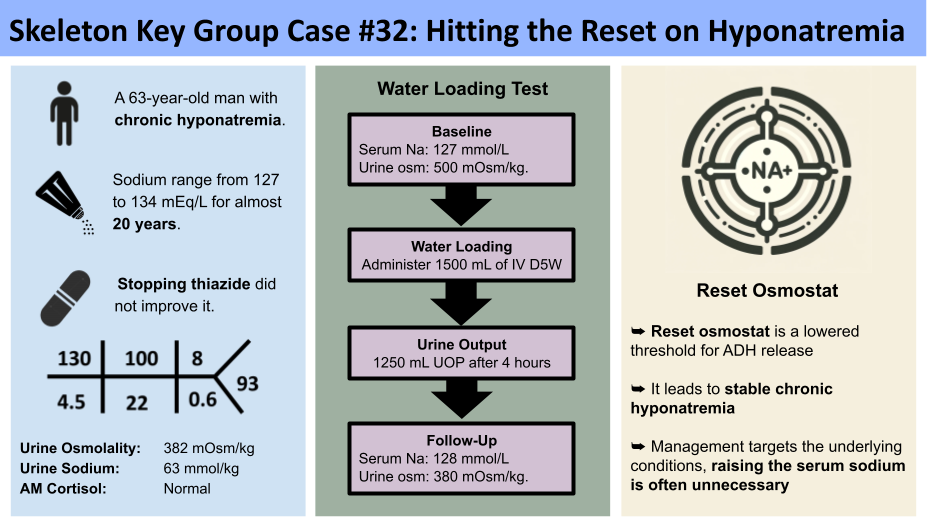
A 65-year-old man with a history of hypertension, alcohol and tobacco use presented to the outpatient nephrology clinic for evaluation of hyponatremia. A review of prior sodium levels in the medical record ranged from 127 to 134 mEq/L over the last 20 years. Previously he was treated with hydrochlorothiazide, but changing that to lisinopril and amlodipine did not correct his sodium. He did not have a family history of kidney disease. He ate a balanced diet that was low in sodium and contained fruits and vegetables. He drinks 1200-1800 mL of water and 1775-2500 mL of beer a day (5-7 cans per day). Home medications include amlodipine, lisinopril, omeprazole, and a multivitamin.
Vital signs: BMI 30kg/m2 blood pressure 142/83 mm Hg, heart rate 92 bpm
Physical exam: The patient was well-nourished and calm. The heart had a normal rate and regular rhythm without murmurs or gallops. The lungs were clear bilaterally. No edema was noted in lower extremities. He was alert and oriented x 4 with a normal gait.
B. The Labs
Serum osmolality 269 (ref. 275-295 mOsm/kg)
Urine Sodium 63 mmol/kg
Urine Osmolality 382 (ref. 50-1,200 mOsm/kg)
AM Cortisol 6.7 (ref. 3.7 – 19.4 mcg/dL)
FeUric Acid 5.5%
Serum Uric acid 4.3 (ref. 3.5 -8.0 mg/dL)
TSH 1.32 (ref. 0.35 – 4.94 lU/mL)
C. The Workup
Hyponatremia is defined as a serum sodium concentration below 135 mmol/L. “True” hypotonic hyponatremia is a consequence of an increase in total body water relative to sodium. Normally, hypotonicity suppresses ADH allowing the production of a large amount of hypotonic urine. The approach to hyponatremia is shown here:
Diagnostic approach to hyponatremia
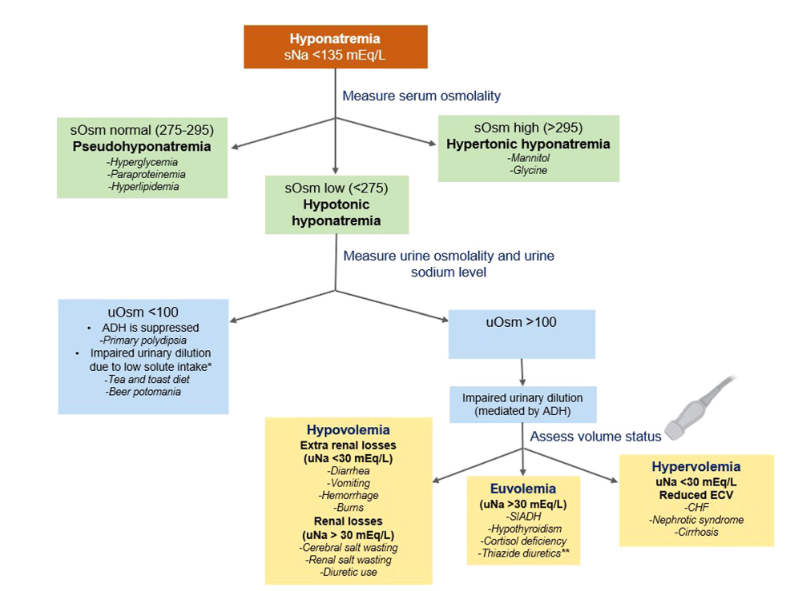
An approach to hyponatremia. We note that this figure does not include hyponatremia due to oliguric kidney failure. Image Credit: Bhasin-Chhabra et al.
The first step is to assess serum osmolarity. Isotonic (275-295 mOsm/kg) or hypertonic (>295 mOsm/kg) hyponatremia states should always be ruled out. For more information on isotonic/hypertonic hyponatremia please see this SKG case. The patient’s serum osmolality is 269 mOsm/kg, indicating true hypotonic hyponatremia.
The next step would be evaluating the urine osmolality to assess ADH activity. A urine osmolality <100 mOsm/kg indicates intact urinary dilution and hyponatremia due to an ADH independent etiology (ADH is maximally suppressed). Hyponatremia that is ADH independent can be due to primary polydipsia or low solute intake (sometimes referred to as tea and toast or beer potomania). We noted in the history that the patient has alcohol dependence, drinking 5-7 cans of beer per day. Our patient’s urine osmolality is 382 mOsm/kg, which indicates impaired urinary dilution that is ADH dependent.
The final step is to evaluate the urine sodium which is used to assess the activity of the renin-angiotensin aldosterone system (RAAS). A urine sodium less than 30 suggests increased RAAS activity indicative of volume depletion or volume overload. The urine sodium of 63 mmol/kg, in addition to the patient’s unremarkable history and physical examination, points us away from hypo/hypervolemia. In euvolemia, hormonal evaluation with serum cortisol for adrenal insufficiency is an important step. The TSH and morning cortisol were normal in this patient.
The workup suggests SIADH… but for 20 years?
At this point in delineating the etiology of hyponatremia, SIADH is a reasonable diagnosis to consider given the findings of a hypotonic hyponatremia with increased urine osmolality (> 100 mOs/kg) and urine sodium (> 30 mEq/L). One must rule out any secondary cause of SIADH, such as pain, malignancy, or medications. In this case, after careful review of his medication list, he was taking lisinopril, which has been reported as a rare cause of SIADH. However, the patient’s lisinopril was stopped for 2 weeks, but repeat sodium remained at 129 mmol/L. What is unique about our patient is he was hyponatremic for almost 20 years. This case is atypical for SIADH given the patient’s long history of stable, and mild, hyponatremia despite at times high levels of fluid intake. In addition, the FeUric acid was less than 10%, which is not consistent with SIADH.
Reset osmostat syndrome. Reset osmostat is a condition in which the threshold for ADH release and thirst regulation is shifted downwards, resulting in mildly reduced serum sodium levels (usually between 125 and 135 mEq/L), which remains stable despite changes in water intake. In response to a water load, individuals with a reset osmostat will typically excrete more than 80 percent of the excess water within four hours, similar to the response observed in normal subjects. This differs from SIDAH, where the ability to excrete excess water is impaired due to the persistent release of ADH.
This modified figure shows the normal physiological response—the normal “osmostat”—to changes in plasma osmolality and secretion of ADH compared with reset osmostat. Image Credit: www.physiologyweb.com/
The Water Load Test
A water load test usually requires 10-15 ml/kg of oral or intravenous water. A healthy individual should excrete 80% or more of the ingested water load due to the suppression of ADH within four hours. However, in the setting of SIADH, the hormone is not able to be suppressed so urine excretion is reduced to 30-40% of the ingested water load. In reset osmostat the ADH regulation is normal but the threshold for its release is lower. That is why a patient with a reset osmostat will respond to the free water load in the same manner as a healthy individual.
Here are the results for our patient’s water loading test:
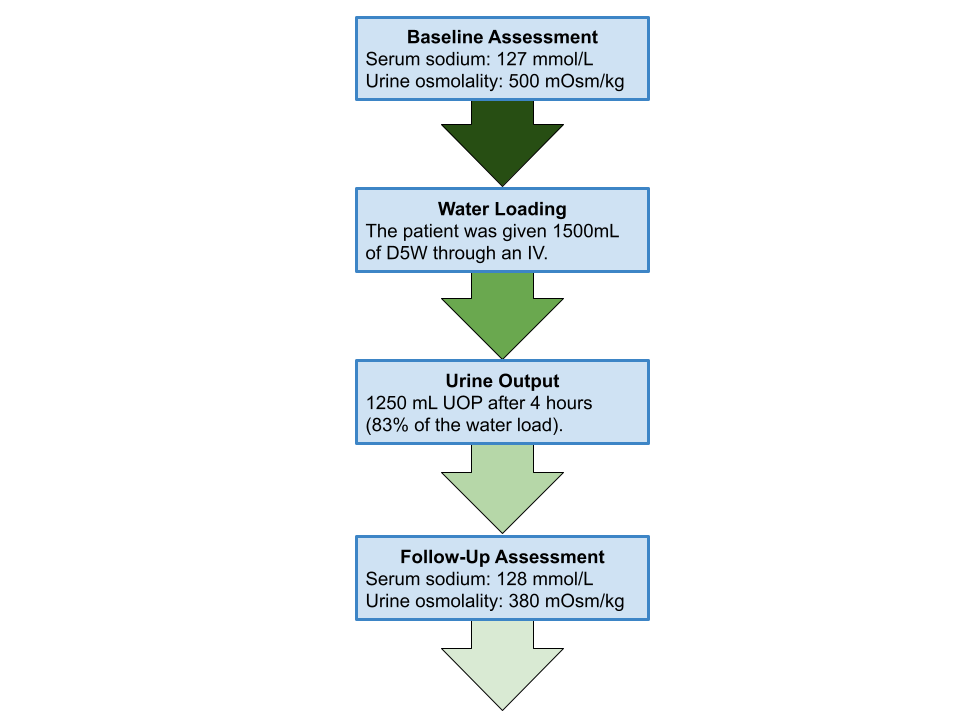
In response to the water loading test, the patient’s urine osmolarity decreased and urine output increased, accounting for over 80% of the administered water load. The patient’s serum sodium, however, remained 127-128 mmol/L. He demonstrated an intact ability to dilute urine, which is consistent with reset osmostat and not SIADH.
D. The Diagnosis
Chronic hypotonic euvolemic hyponatremia due to reset osmostat syndrome
The pathophysiology of reset osmostat is currently unclear. It is hypothesized that an alteration in the osmoreceptor cell metabolism may lead to reset osmostat syndrome. It is associated with advanced age, cerebral hemorrhage, alcohol dependence, malignancy, and Pneumocystis jirovici pneumonia. In pregnancy, a physiological decrease in osmotic thresholds for thirst and ADH release results in increase in water intake and fluid retention. The diagnosis of reset osmostat can only be definitively made by performing a water load test.

Management
Providers should not try to treat the hyponatremia found in reset osmostat as the osmoreceptor is functioning normally. Attempting to raise the sodium will further stimulate ADH and thirst. This can lead to a further lowering of the sodium. Patients should be monitored for symptoms related to hyponatremia. Although chronic hyponatremia can be associated with falls and cognitive deficits, there is currently no evidence tying these symptoms to reset osmostat.
In this case, our patient was educated about his condition and continued routine medical care with his primary care physician. There was no restriction of fluid intake. We counseled him on tobacco and alcohol use. We recommended that the patient avoid thiazides, which may impair urinary dilution and worsen hyponatremia, although there is no empirical data supporting this course of action in the context of reset osmostat. Lastly, the patient will report any new symptoms without delay.
E. Take home points
- Reset osmostat is a disorder characterized by a lower threshold for ADH release, leading to a reduced serum sodium concentration that is stable over multiple measurements
- A water loading test, which tests an individual’s ability to dilute their urine, can differentiate reset osmostat from SIADH
- Patients with reset osmostat will excrete more than 80% of the free water load within 4 hours of ingestion
- The hyponatremia related to reset osmostat does not need to be treated in most cases. Treating any underlying conditions is most important.
Editors and Reviewers: Jefferson L. Triozzi, Raad Chowdhury, Chi Chu, Joel Topf, Margaret DeOliveira, Matthew A. Sparks
Visual Abstract