Case
The patient history in this post is fictitious, but represents how a patient with high output cardiac failure and pulmonary hypertension post kidney transplantation might present.
A 73-year-old man with kidney failure secondary to unknown etiology was on hemodialysis for about two years before receiving a deceased donor kidney transplantation (DDKT). His hemodialysis access was a left arm brachiocephalic arteriovenous fistula (AVF). Post kidney transplant, his creatinine improved from 4 mg/dL to 1.0 mg/dL. A year later, he developed aneurysmal dilatation of his AVF along with dyspnea, lower extremity edema, activity restriction and an elevated creatinine of 2 mg/dL. He was evaluated in the transplant clinic and further investigations were pursued. Echocardiogram revealed a left ventricular ejection fraction of 46%, right ventricular systolic pressure (RVSP) of 59 mmHg and moderate to severe mitral regurgitation. Transplant kidney doppler did not reveal renal artery stenosis and the resistive index (RI) at the anastomosis was 0.85 (normal RI is less than 0.7 to 0.8). AVF ultrasound revealed an aneurysmal AVF with inflow volume (Qa) of 2.2 L/min. He was referred to cardiology and vascular surgery for further management. Cardiac catheterization revealed pulmonary hypertension with RVSP of 65 mm Hg, pulmonary artery pressures (PAP) of 70/30 mm Hg, mean PAP of 43 mm Hg, mean pulmonary capillary wedge pressure (PCWP) 25 mm Hg and cardiac output (CO) of 8.69 L/min. He was diagnosed with AVF mediated high output cardiac failure (HOCF), pulmonary hypertension (PH) and underwent AVF ligation with aneurysmal sac and fistula resection. During post operative visits, he reported improved dyspnea and edema. He is not using any diuretics, his exercise capacity has significantly improved and the most recent creatinine was 1.2 mg/dL.
Discussion
Cardiovascular disease (CVD) in kidney transplant recipients (KTRs) contributes to 50-60% of post transplant deaths and CVD can be secondary to coronary artery disease, PH, congestive heart failure, left ventricular hypertrophy or myocardial ischemia. Of these, PH and HOCF can be mediated by AV access.
- Why does AV access lead to cardiac complications?
Following the creation of an AV access, there is reduction in systemic vascular resistance (SVR) with increase in CO and elevations in cardiac chamber pressures. Overtime high cardiac chamber pressures lead to HOCF. Below table provides a timeline of hemodynamic progressions.
| Timeline | Hemodynamic changes |
| Acute changes (immediate) | Decrease in SVR Increase in CO |
| Subacute changes (within 2 weeks) | Increase in RA, RV, PA LVEDP |
| Chronic changes(over weeks and months) | RV dysfunctionLV eccentric hypertrophyLV dysfunction |
It is important to exclude other causes of HOCF such as obesity, pregnancy, cirrhosis, thyrotoxicosis, anemia, paget’s disease, AV malformations, psoriasis, hypercapnia and myeloproliferative disorders. These conditions can be due to low SVR or increased blood volume or high metabolic rates.
- Do all AVFs cause HOCF?
Not all AVFs lead to HOCF but the below risk factors increase the odds of developing HOCF.
- Upper arm AVF- Brachiocephalic fistulas Qa can be double the radiocephalic fistulas Qa. Higher access flow rates confer higher risk of worsening heart failure.
- Male sex
- History of prior vascular access surgery
- Vascular access blood flow (Qa) >2.0 L/min
- How are AVF-mediated HOCF, PH diagnosed?
HOCF can be diagnosed by echocardiographic findings of elevated cardiac chamber pressures and cardiac dysfunction. Confirmation is by cardiac catheterization findings of CO greater than 8 L/min, PCWP > 14 mm and LVEDP > 16 mm Hg.
PH is diagnosed by right heart catheterization findings of elevated mean PAP >20 mm Hg. Manual compression of AV access under therapeutic heparinization shows improvement in pulmonary hemodynamics with decrease in heart rate (Branham’s sign)
- How are HOCF and PH managed?
HOCF and PH are managed by correcting anemia, administering diuretics for volume control and by pharmacological management of heart failure. Definitive management involves AV access flow restriction banding through MILLER technique (Minimally Invasive Limited Ligation Endoluminal-Assisted Revision) or AVF ligation, revision procedure through DRIL (Distal Revision with Internal Ligation) or RUDI (Revision Using Distal Inflow) procedures. MILLER is a banding technique that decreases flow by decreasing the radius at a specific point and thus reduces access flow and pressure. DRIL is a two-step procedure that consists of arterial ligation just distal to the anastomosis, and the creation of an arterial bypass (using either expanded polytetrafluoroethylene (ePTFE) or a reversed saphenous vein) from the artery proximal to the anastomosis to the artery distal to the ligation. RUDI procedure entails fistula ligation at its origin followed by creation of a bypass from a more distal arterial source to the venous limb to reestablish the fistula.
- To ligate or not to ligate?
Current guidelines do not address whether AVFs should be ligated in KTRs when they are no longer in use and clinical studies have not demonstrated a reduction in CV-related mortality in patients whose AVF were ligated. However, when high flow AVFs are associated with HOCF such as our patient, reduction of flow through ligation is appropriate.
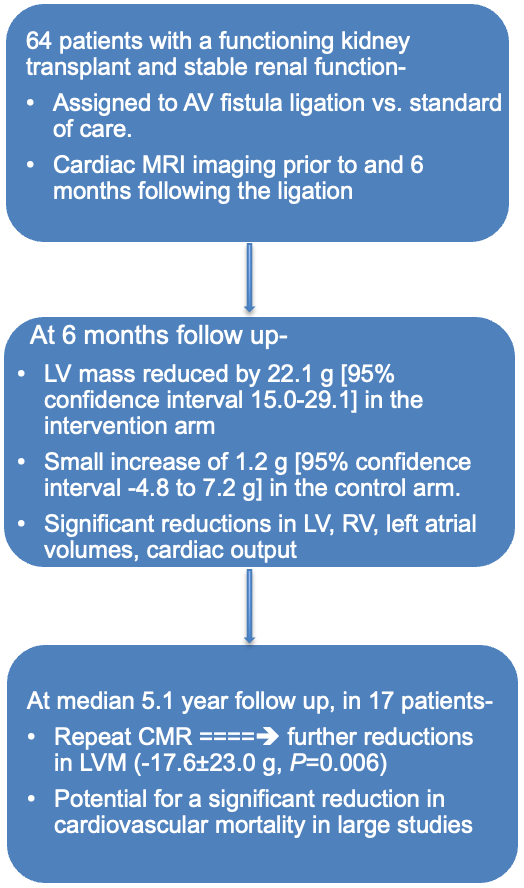
Below is a summary of KTRs with stable allograft function that underwent AVF ligation and the investigators studied changes in cardiac MRI at 6 months and 5.1 years of follow up. There was reduction in left ventricular mass noted on cardiac MRI in the intervention arm. We believe that larger and long term studies will need to be performed to evaluate the role of AVF ligation in KTRs for potential reduction in CVD related morbidity and mortality.
Take home points
- CVD is a major cause of morbidity and mortality in kidney failure KTRs.
- AVF mediated HOCF, PH are diagnosed based on CO, mean PAP on cardiac catheterization.
- AVF ligation in asymptomatic KTR is an evolving field
Reviewed by Matthew A. Sparks. And Margaret DeOliveira