Welcome to the 38th case of the Skeleton Key Group, a team of nephrologists from around the world who build a periodic education package for the Renal Fellow Network.
Author: Eric S. Chai (@Eric__Chai)
A. Stem
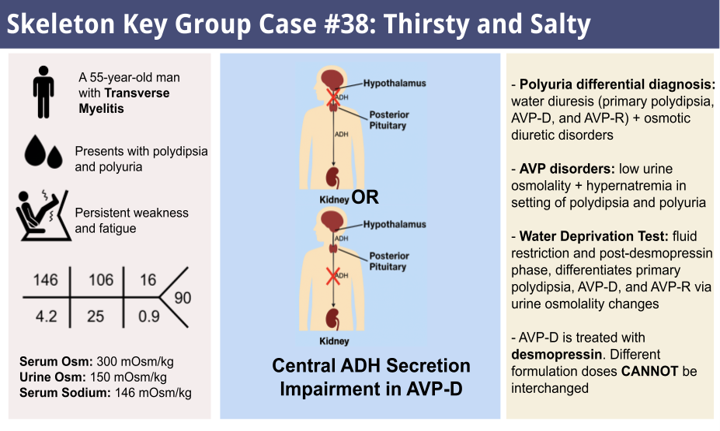
A 55-year-old man with a past medical history of idiopathic transverse myelitis, diagnosed 5 years ago, and neurogenic bladder dysfunction with a chronic indwelling Foley catheter presents to the emergency department for a fall and femur fracture. During the patient interview, he reports severe thirst and excessive urination for the last 6 months. Notably, the patient has multiple twelve-packs of bottled water at his bedside and is constantly drinking, even awakening at night to quench his thirst. This is corroborated by his wife, who says he is “thirsty all the time,” requiring constant changing of his urinary bags.
Evaluation reveals the following vital signs, which remained stable throughout the patient’s stay:
- Temperature: 98.3 ℉
- Blood Pressure: 128/76 mm Hg
- Heart Rate: 82 bpm
- Respiratory Rate: 16/min
- Oxygen Saturation: 98% on room air
Physical Examination:
- General: Tired but well-nourished
- HEENT: normal appearing oral mucosal membranes.
- Neck: No jugular venous distention
- Heart: No murmurs
- Lungs: Clear to auscultation bilaterally, not in respiratory distress
- Abdomen: Soft, non-tender, non-distended
- Skin: No bruising, discoloration, or other abnormalities
- Extremities: no edema or range of motion abnormalities
- Neuro: Diminished sensation to light touch below the neck; bilateral leg weakness
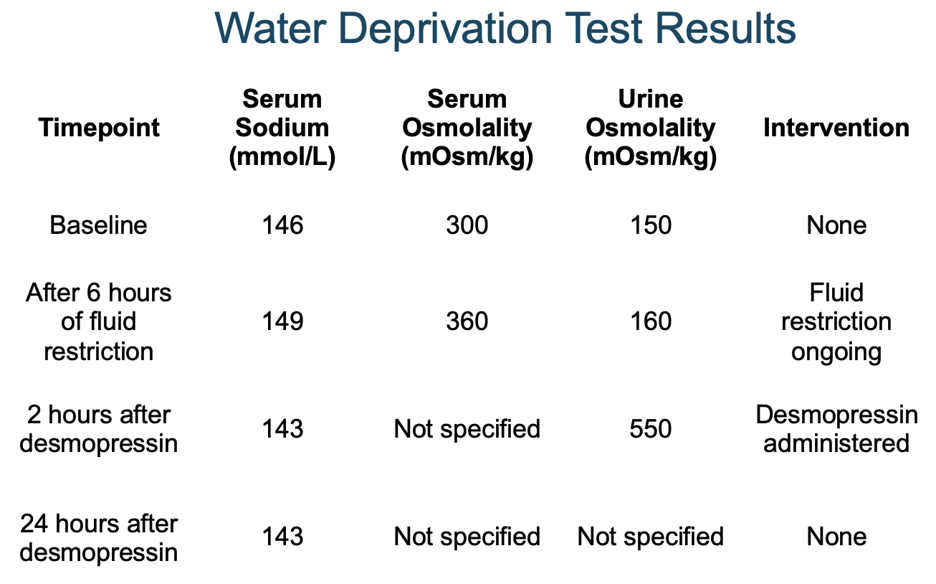
B. Labs
- 24-hour urine output: 5 L
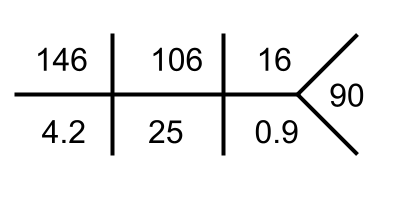
- Serum Osmolality: 300 mOsm/kg
- Urine Osmolality: 150 mOsm/Kg
C. Workup
Why is this patient so thirsty?
In the evaluation of a patient with thirst and polyuria, we must first confirm polyuria and evaluate urine osmolality to distinguish water diuresis from osmotic diuresis.
Polyuria is defined as >3L/day of urine (24-hour urine collection can be used to confirm, normal adult urine output ranges from 1.5-2L/day). Additionally, electrolytes (e.g. Na, K, Cl), proteins, glucose, and other molecules within the urine can be analyzed to gain insight into the underlying cause of excessive diuresis, although we did not obtain those in this case.
Urine osmolality will differentiate water diuresis from osmotic diuresis. Water diuresis describes excessive water secretion in the setting of impaired reabsorption, whereas osmotic diuresis refers to solute-driven water secretion via osmotic pressure into the lumen of nephrons. These can be characteristically distinguished by urine osmolality, with water diuresis exhibiting low readings (<250 mOsm/kg) in contrast to the elevated readings seen in osmotic diuresis (>300 mOsm/kg).
This Case: We have confirmed polyuria, with an elevated serum osmolality (>295 mOsm/kg) and low urine osmolality (<250 mOsm/kg) suggesting a water diuresis, so we need to differentiate between (i) primary over-drinking vs. (ii) a kidney concentrating defect. Three differential diagnoses will come to mind:
- Primary polydipsia [primarily over-drinking]
- Commonly psychiatric or idiopathic, this condition is characterized by excessive water intake, resulting in elevated urine excretion.
- Arginine vasopressin deficiency (AVP-D) [concentration defect]
- Impaired central release of antidiuretic hormone (ADH) results in reduced ability to concentrate urine and retain fluid within the body.
- Arginine vasopressin resistance (AVP-R) [concentration defect]
- Impaired receptor response to ADH results in reduced ability to concentrate urine and retain fluid within the body.
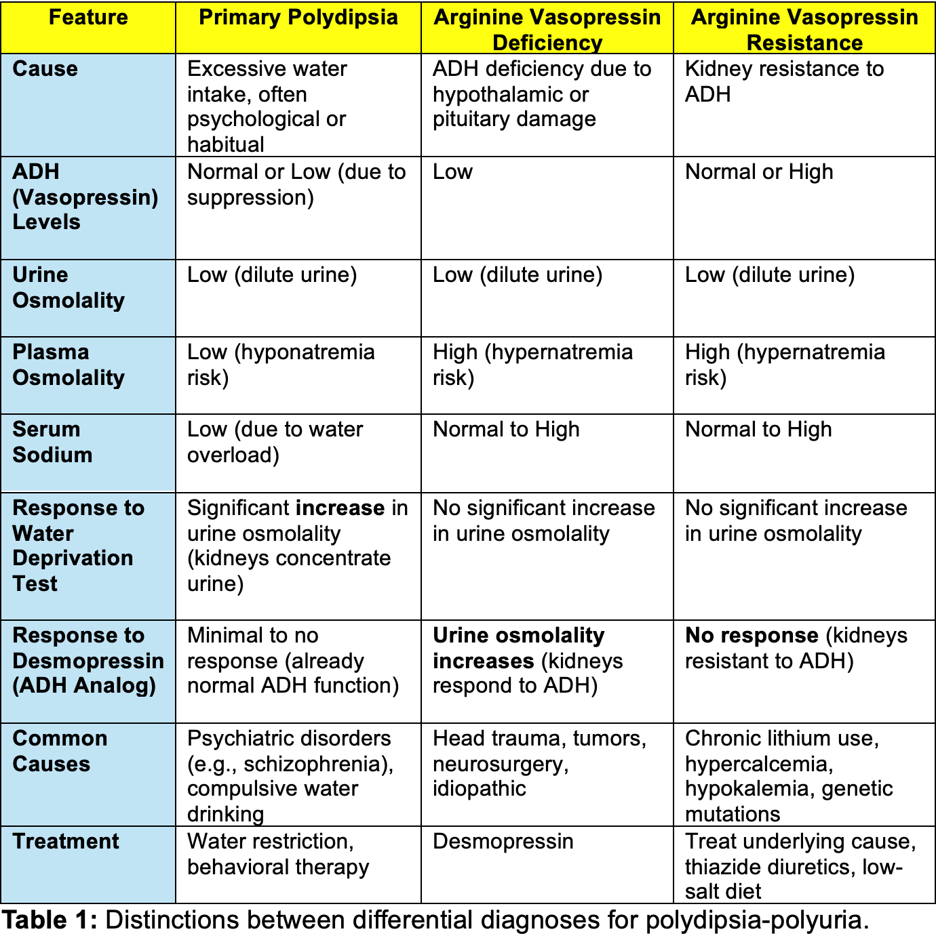
More details about the comparisons made in this table can be found here.
AVP-D and AVP-R were formerly known as central diabetes insipidus and nephrogenic diabetes insipidus respectively; however, the disorders were renamed in 2022 to increase their distinction from diabetes mellitus.
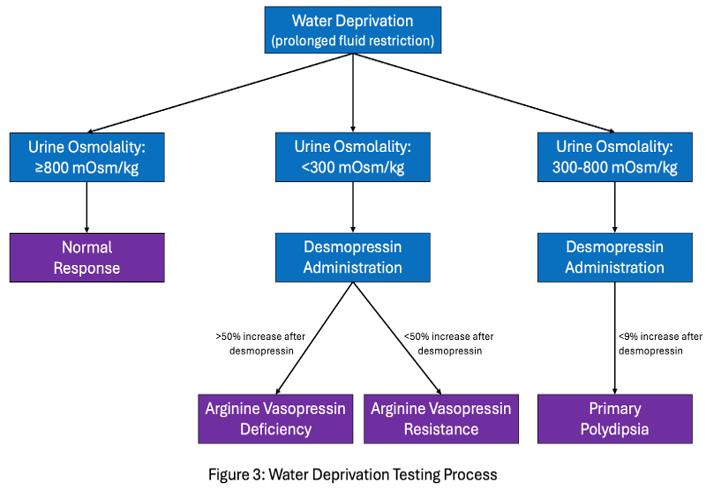
A Water Deprivation Test to get the answer
In the initial workup of a patient experiencing polydipsia and polyuria, one should obtain a reading of body weight, serum sodium, serum osmolality, and urine osmolality. These results will serve as a baseline from which we can perform water deprivation testing [Figure 3]. In water deprivation testing, the patient’s fluid intake is restricted for an extended period of time (usually 8 hours) with vitals, serum sodium, serum osmolality, and urine osmolality being measured in 1-2 hour increments.
Outline of Water Deprivation Test
- Baseline: weight, Na⁺, serum/urine osmolality.
- Deprivation phase (0-8 h)
- Check every 1–2 h.
- Stop if weight ↓ >3 %, Na⁺ >150, or symptomatic hypovolemia.
- If urine osmolality ≥ 800 mOsm/kg at any point → AVP intact → stop.
- Desmopressin 2 µg IV/IM
- Resume drinking ad lib.
- Re-check urine osmolality at 1–2 h.
- ↑ >50 % is AVP-D.
- ↑ <50 % is AVP-R.
A note on copeptin
The use of copeptin has been proposed as a way to better distinguish primary polydipsia from AVP disorders (although it was not used in our case). Copeptin is a segment within the arginine vasopressin pro-hormone that can be measured without the technical difficulties associated with direct circulating arginine vasopressin (AVP) hormone measurement. In individuals with primary polydipsia, ADH levels are low but can be induced by hypertonic saline infusion. Hypertonic saline, however, has no or minor effects on AVP levels in AVP-D, AVP-R, or physiologically normal patients. 250 mL of 3% saline is initially administered at 0.15 mL/kg/minute. Every 30 minutes, blood samples for plasma osmolality, sodium, urea, and glucose are obtained until sodium levels (monitored using venous blood gas analysis) reach 150 mmol/L. Then, a final blood sample for plasma copeptin is measured. A plasma copeptin level of 4.9 pmol/L or less indicates AVP-D (partial or complete), whereas a value greater than 4.9 pmol/L indicates primary polydipsia. Copeptin hypertonic saline testing has been proven superior to the previously described indirect water deprivation test method in distinguishing primary polyuria from AVP-D. Additionally, baseline copeptin levels can be used to distinguish partial/complete AVP-R (if greater than 21.4 pmol/L) and complete AVP-D (less than 2.6 pmol/L).
Diagnostic Testing for Diabetes Insipidus
*Note: 300-800 mOsm/kg urine osmolality following water deprivation could be indicative of partial AVP-D or AVP-R if there is less than 50% increase in urine osmolality with desmopressin administration. This can at times be hard to distinguish from primary polydipsia using water deprivation testing if the AVP disorder is particularly mild.
D. Diagnosis
Arginine vasopressin deficiency was suspected in this patient with severe thirst and polyuria, a high serum osmolality, and an inability to concentrate his urine during water deprivation that was corrected with subsequent desmopressin administration.
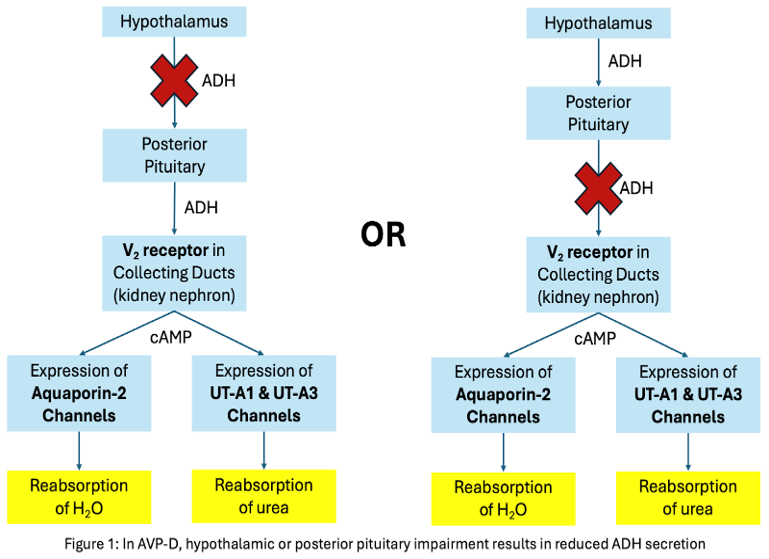
Let’s review the pathophysiology of AVP-D a little closer.
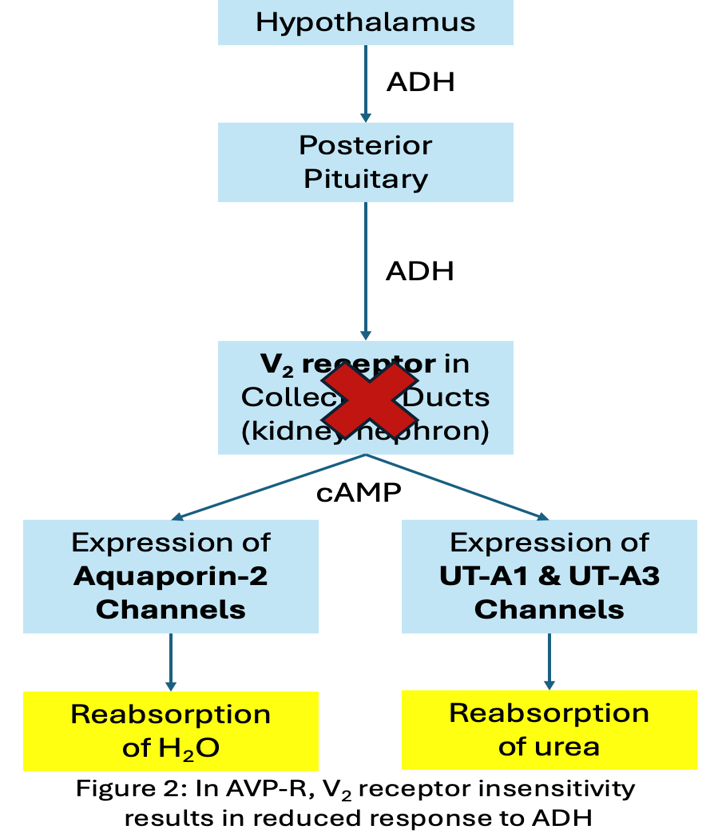
The pathophysiology of both forms of arginine vasopressin dysfunction centers around defective ADH function. ADH is released in response to changes in blood osmolarity via osmoreceptor signaling and volume depletion via baroreceptor response. ADH then stimulates water reabsorption through aquaporin channels in the principal cells of the distal nephron via an intracellular cAMP pathway. AVP-D is characterized by hypothalamic or posterior pituitary dysfunction resulting in diminished ADH secretion [Figure 1], whereas AVP-R is the result of impaired ADH response caused by dysfunctional renal V2 receptors [Figure 2].
In arginine vasopressin deficiency, hypothalamic or posterior pituitary impairment results in reduced ADH secretion [Figure 1]. However, in arginine vasopressin resistance, V2 receptor insensitivity results in reduced response to ADH.
Etiologies: Could Transverse Myelitis Be the Culprit?
Always consider underlying causes to AVP-D (autoimmune, tumors, head trauma, or infiltrative diseases such as Langerhans cell histiocytosis and sarcoidosis).
This patient has transverse myelitis is an inflammatory disease of the spinal cord that is often associated with autoimmune diseases. Neuromyelitis Optica Spectrum Disorder (NMOSD) is particularly associated with longitudinally extensive transverse myelitis, characterized by anti-aquaporin-4 antibodies that target astrocytes in both the spinal cord and hypothalamus. Thus, AVP-D via hypothalamus injury or even AVP-R from aquaporin destruction may be interesting considerations. NMOSD has been associated with higher rates of AVP-D; however, neither the mechanism behind the association nor the association with AVP-R have been elucidated. Notably, transverse myelitis-associated systemic lupus erythematosus flare ups have also been linked to AVP-D, likely via antiphospholipid antibody damage. Endocrine structures like the hypothalamus and posterior pituitary are particularly susceptible to autoimmune destruction and lymphocytic infiltration, perhaps accounting for the significant correlation observed between idiopathic AVP-D and autoimmunity.
E. Followup
Arginine vasopressin deficiency is usually managed effectively using desmopressin. Desmopressin is an ADH analog that is most commonly administered in an intranasal liquid form, oral tablet form, or parenteral formulation. At first, AVP-D treatment should be targeted at reducing nocturia in order to allow for uninterrupted sleep. This means initially administering desmopressin at bedtime, starting with the minimum dosage and titrating upward. After control of nocturia is achieved, partial control of daytime diuresis may then be pursued. Note that aggressive treatment with desmopressin may result in hyponatremia from excessive ADH activity.
Note:
Patients with AVP-D who receive Intravenous fluid replacement (dextrose + water) prior to correction of their polyuria may develop severe hyperglycemia. This is especially pertinent for patients with AVP-D who are intubated or otherwise unable to consume oral fluids. Intravenous fluid replacement should thus be limited with close monitoring of serum glucose. This is not pertinent to the current case but is an important note in AVP-D treatment.
For AVP-D, this patient was initiated on 0.05 mg desmopressin oral tablets BID, which was titrated up to 0.1 mg over course of admission (0.05 mg titration increments recommended). A low solute diet was also initiated in order to reduce required urination volume for solute excretion. Polyuria reduced dramatically upon discharge and serum sodium remained in normal range (around 143 mmol/L) following intervention. Rheumatology was consulted to evaluate transverse myelitis and assess status of autoimmune regulation with concern autoimmunity may have contributed to AVP-D development.
F. Take home points:
- The differential diagnosis of polyuria includes water diuresis disorders (e.g. primary polydipsia, AVP-D, and AVP-R) and osmotic diuresis disorders (e.g. uncontrolled diabetes, uremia, serum electrolyte disturbances, etc.).
- An AVP disorder should be suspected when a patient has polyuria and polydipsia in the setting of low urine osmolality (<250 mOsm/kg), hypernatremia (>145 mmol/L), and unresponsiveness to fluid restriction.
- A water deprivation test includes a fluid restriction phase and post-desmopressin phase, allowing us to differentiate primary polydipsia, AVP-D, and AVP-R via changes in urine osmolality across each phase.
- Transverse myelitis and autoimmunity are associated with higher rates of AVP-D. This may be due to injury to the vulnerable hypothalamus and pituitary.
- AVP-D is treated with desmopressin.
Editors: Jefferson L Triozzi, MD MSCI, Carolina Mendez, Santhoshi Bavi, MBBS, Chi Chu, Joel Topf, Raad Chowdhury, MD FASN, Matthew A. Sparks, MD, Srinath Yadlapalli, M.D