Welcome to the fifth case of the Skeleton Key Group, a team of twenty odd nephrology fellows who work together to build a monthly education package for Renal Fellow Network. The cases are actual cases (without patient identifying information) that intrigued the treating fellow.
Case 5: Written by Jose Mena
Visual Abstract: Dhwanil Patel
A. The Stem
A 65 year-old with a history of hypertension, hyperlipidemia, insomnia, anxiety and osteoporosis presented to the Emergency Department after ingesting an unknown substance. The patient lives alone and was found down on the floor, breathing, and unresponsive.
Home medications: amlodipine, atorvastatin, trazodone.
Social history: Widowed, retired. No history of smoking or use of illicit drugs. Drinks a glass of wine per week.
Vital signs: Blood pressure: 107/59 mm Hg and on repeat 77/49; Heart rate: 56/min, regular; Respiratory rate 18 breaths/min; Temperature 84.6 Fahrenheit. Weight: 55 Kg.
On exam, the patient was unresponsive (Glasgow Coma Scale 3). Skin was dry and cool. Lungs had good airway entry with scattered rhonchi. In the Emergency Department (ED), the patient was intubated for airway protection. 2 liters of warmed normal saline were administered.
B. The Labs
Labs from 3 months prior to the presentation:

In the ED, the patient received 100 mEq of sodium bicarbonate and was started on a sodium bicarbonate infusion at the rate of 125 mL/hour. In addition, a single dose of intravenous fomepizole 830 mg (15 milligram/kilogram loading dose) was administered. Propofol and norepinephrine were also started.
C. Differential Diagnosis: High Anion Gap Metabolic Acidosis
What do you think is going on? What is the differential diagnosis for a High Anion Gap Metabolic Acidosis?
- Carbon Monoxide, Cyanide
- Aminoglycosides
- Toluene
- Methanol
- Uremia
- Diabetic Ketoacidosis (DKA)
- Paraldehyde, Phenformin
- Iron, Isoniazid
- Lactic acidosis
- Ethylene Glycol
- Salicylates
Here’s the GOLDMARK mnemonic:
- Glycols (ethylene and propylene)
- Oxoproline
- L-Lactate
- D-Lactate
- Methanol
- Aspirin
- Renal failure
- Ketoacidosis
D. More Data
| Lactate | >31 mmol/L |
| Calcium | 10.4 mg/dL |
| Serum toxicology | Negative |
| Urine toxicology | Negative |
| INR | 1.4 |
| Albumin | 3.6 g/dL |
| Creatine phosphokinase (CPK) | 253 U/L |
| Serum osmolality | 354 mOsm/KgH2O |
| Venous blood gas | pH: 6.77 / PCO2: 20 / PO2: 165 |
| Urinalysis | Ketones 1+, Blood 2+ |
| Urine osmolality | 635 mOsm/KgH2O |
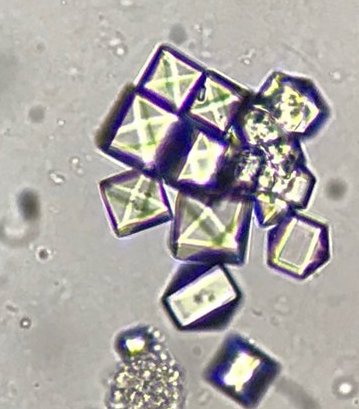
| Urine sediment | Calcium oxalate monohydrate crystals |
E. Final Diagnosis & Management
Ethylene Glycol Ingestion, Acute Kidney Injury, Lactic Acidosis, Hypernatremia, Shock
The patient was diagnosed with ethylene glycol ingestion, acute kidney injury, hypernatremia, lactic acidosis, and shock. She required emergent dialysis and was started on fomepizole.
1. Toxicology
Ethylene glycol is absorbed very fast after oral administration. After ingestion, It reaches peak levels in approximately 1 to 4 hours and the metabolism is done in the liver by cytosolic enzymes. (Fig 2)
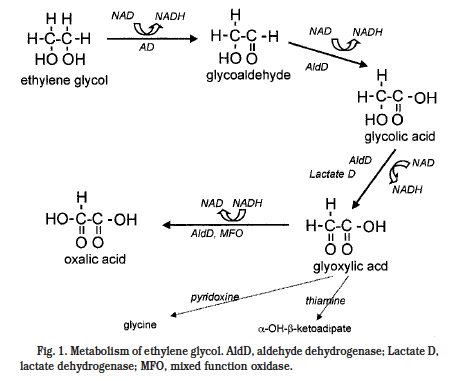
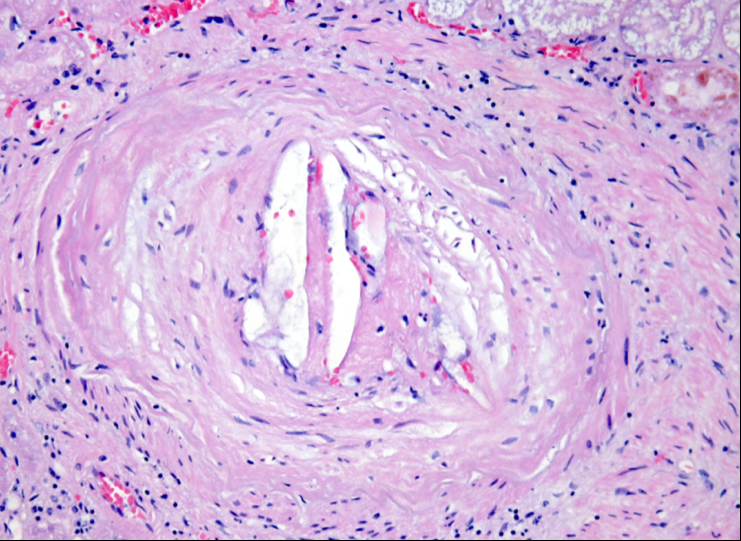
Ethylene glycol toxicity is driven by its metabolites including: glycolic acid, glyoxylic acid, and oxalic acid. All of them play a part in the development of metabolic acidosis with a high anion gap. The main toxic effects in our system are severe metabolic derangements and acute tubular necrosis due to deposition of calcium oxalate crystals.
Some patients may have hypocalcemia resulting from calcium binding to oxalate to form calcium oxalate crystals. However, this is not found in all cases of ethylene glycol poisoning or in all cases with calcium oxalate crystalluria
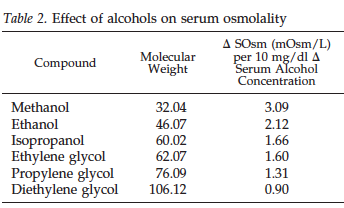
2. Effect of Alcohols of Serum Osmolality and Osmolal Gap
The normal serum osmolality level is around 285 to 290 mOsm/L. It can be calculated using the following equation:
You can also calculate it with international units (mmol/L):
Calculated Serum Osm = (2 x serum [Na]) + [glucose] + [urea] + (1.25 x [ethanol])
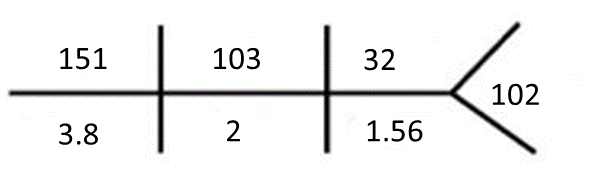
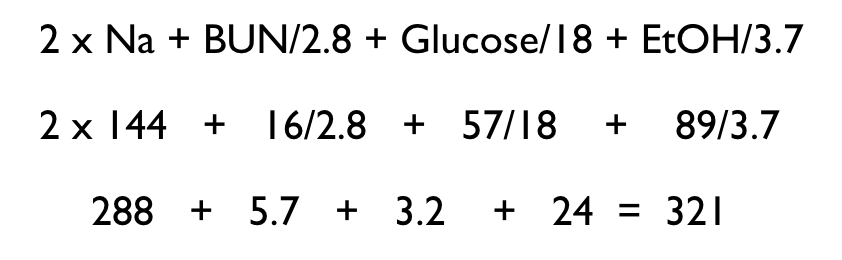
In our patient: Serum osm (US units) = (2 × Na + (BUN / 2.8) + (glucose / 18) + (ethanol / 3.7)
Calculated serum osmolality
(2 x[151]) + [32/2.8] + [102/18] + (0/3.7])
(302) + [11.4] + [5.6] + (0) = 319
Measured serum osmolality: 354
Osmolal gap: (354) – (319)
Osmolal gap: 35 mOsm/Kg
The serum osmolality is measured by freezing point depression and is considered normal when it is within 10 mOsm/L of the calculated serum osmolality. A gap between these two is seen in the presence of alcohols and other low molecular weight substances in the serum. These molecules raise the measured serum osmolality above of the calculated serum osmolality creating an osmolal gap. (Fig 3)
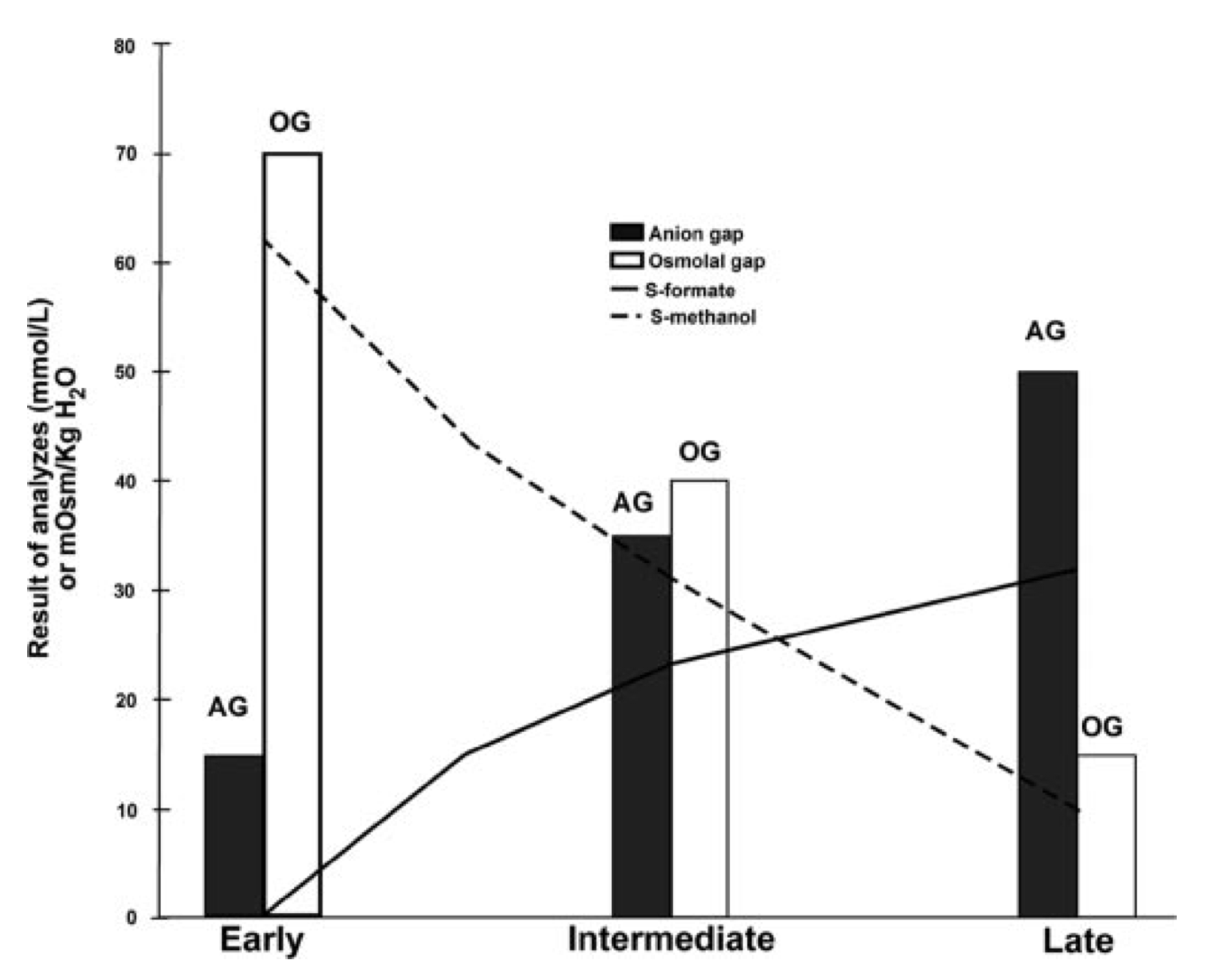
An osmolal gap greater than 20 mOsm/L is indicative of increased concentrations of one of these alcohols in the blood; however, it does have limitations and can be either a false positive or false negative. The osmolal gap when used as a screening test for toxic alcohol poisoning has a sensitivity between 85-90% and a specificity of 22-50%. Therefore, a normal osmolal gap does not rule out alcohol poisoning. In our patient, the osmolal gap was 35. An important concept to understand is how the osmolal gap starts high and then falls after intoxication, while the anion gap starts normal and increases over time. See Fig 4.
The plasma osmolal gap estimates the quantity of uncharged molecules and is increased in the presence of the parent (uncharged) alcohol (methanol in the figure; ethylene glycol in this case). As toxic alcohol is metabolized it is broken down into anions (formate in the figure; glycolate, glyoxylate and oxalate in this case of ethylene glycol toxicity). Since these anions are accompanied by a cation (mostly sodium), they are accounted for in the osmolal gap formula by doubling the sodium concentration. So they do not contribute to the calculated osmolal gap. They do, however contribute to the anion gap which grows as the toxic alcohol is metabolized. So the pattern in ethylene glycol, methanol and most other toxic alcohols is the patient initially has a high osmolal gap but over time the osmolal gap falls while the anion gap rises.
3. Basic principles of management
Gastric absorption of ethylene glycol is very quick. Gastric lavage could be considered only if initiated within 1 hour of ingestion; it has not been documented to help. The use of activated charcoal is not recommended because it does not bind ethylene glycol.
Intravenous administration of a base solution like bicarbonate, corrects the metabolic acidosis and it can improve the urinary excretion of ethylene glycol and its metabolites. Also, it may prevent the deposition of oxalate in the tubules and subsequent renal failure.
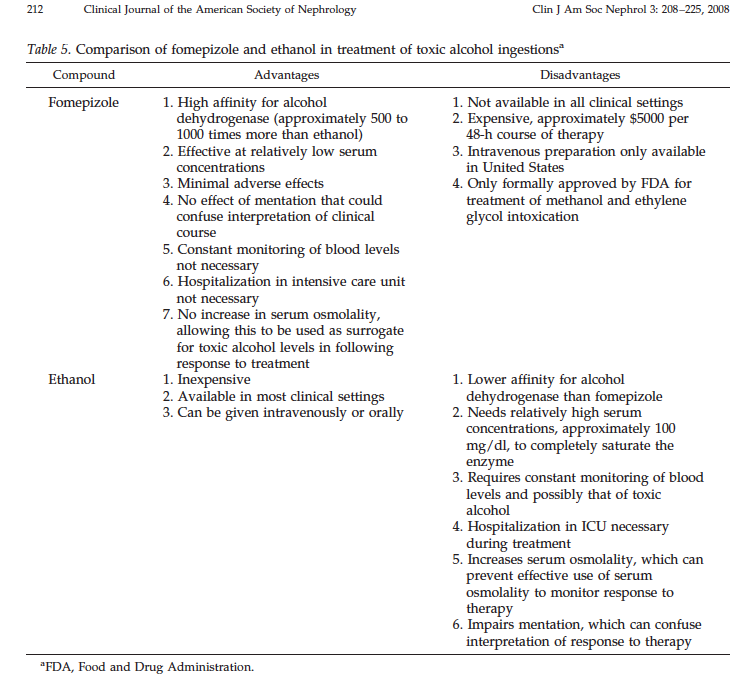
One of the cornerstones in management of toxic alcohol poisoning is to prevent their metabolism into their toxic metabolites with either ethanol or fomepizole. Despite the fact that ethanol has not been approved by the Food and Drug Administration (FDA) for this, it has been used in the treatment of methanol and ethylene glycol intoxication for decades.
Fomepizole (Fig 5), the antidote of choice has an affinity for alcohol dehydrogenase (ADH) approximately 500 – 1000 times higher than ethanol and it can inhibit ADH at a much lower serum concentration. It is the only FDA approved treatment of methanol and ethylene glycol poisoning.
There are only a few small studies that provide information about pharmacokinetics of fomepizole. Some of these case reports mention that hemodialysis eliminates important amounts of this drug so the dosing schedule should change as seen in Fig 5.

Some clinicians favor skipping dialysis and managing the patient just with fomepizole in patients without:
- Acute kidney injury
- Severe acidosis (pH < 7.25)
- Large anion gaps
- Ethylene glycol concentrations > 50 mg/dL
- Electrolyte abnormalities
However, hemodialysis needs to be considered in every patient with hemodynamic instability despite aggressive therapy in confirmed cases of ethylene glycol or any other alcohol poisoning. It is always indicated with considerable metabolic acidosis (pH < 7.25), electrolyte disorders, renal failure, or serum ethylene glycol concentration > 50 mg/dL. Hemodialysis removes ethylene glycol and its toxic metabolites. As in all cases of poisoning and intoxications, the preferred dialysis modality is hemodialysis which effectively removes toxic alcohols because of their low molecular weight, low protein binding, and small volume of distribution.
The table below shows the ideal properties for extracorporeal removal of drugs and toxins with hemodialysis
| Molecular Weight | <500 Da |
| Protein binding | Low (<80%) |
| Volume of distribution | <1 L/Kg |
| Solubility | Water |
| Endogenous Clearance | < 4 mL/Kg/min |
Hemodialysis could be less expensive than management with fomepizole. Despite this, the use of hemodialysis is related to a higher probability of complications and only patients with clear indications should be started on this treatment.
Take Home Messages
- Stick to one of the mnemonics (GOLDMARK or CATMUDPILES) for your differential diagnosis of high anion gap metabolic acidosis
- Calculate osmolal gap to evaluate for unmeasured alcohols
- Ethylene glycol toxicity is characterized by acute kidney injury, high anion gap metabolic acidosis and the presence of oxalate crystals
- Fomepizole is the antidote of choice in ethylene glycol toxicity
- Always consider hemodialysis in patients with acute kidney injury, severe metabolic acidosis, and high ethylene glycol levels
Other Resources for Drug Poisoning
- EXTRIP (The Extracorporeal Treatments In Poisoning Workgroup)
- Evidence based recommendations on the use of extracorporeal treatments for toxin removal in poisoning
- @ExtripWorkgroup on Twitter
- Good collection of links when NephJC partnered with them
Excellent case!
Si CO2 down chloride in skeleton key? Or is HCO3? So this patinet’s got 2 of CO2 or HCO3? Excellent case!
1) How would she be expected to have drunk ethylene glycol?
2) My community hospital, owned by a system, has centralized osmolality measurement and it is not immediately available.
3) would transfer then be appropriate in all very high anion gap metabolic acidosis cases? I could see being burned by treating this for septic shock and losing the patient from an ingestion.