 The post from Veeraish earlier this week reminded me of this
The post from Veeraish earlier this week reminded me of thispatient who demonstrated an important learning point regarding hypokalemia in hypothermic
patients. A 75 year old woman was found unconscious in her unheated home with
overnight temperatures of -1⁰C. On arrival at the Emergency Department, her
core rectal temperature was a staggering 21⁰C, blood pressure 90/50 and pulse
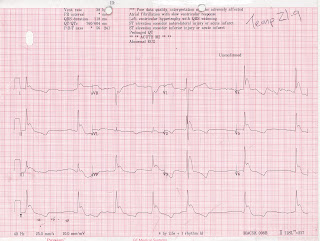
was 28 beats per minute. EKG was classic, demonstrating slow atrial fibrillation,
wide T wave inversion and the characteristic J waves of hypothermia (see Figure; note that the depth of the J wave inflection correlates with the degree of hypothermia). Laboratory values included serum potassium of 1.1 mmol/L, phosphorous
<1 mg/dl, pH 6.95, lactate 8.5 mmol/L, glucose 522 mg/dl. Her renal
function was normal. After some initial warming, repeat potassium was 1.6
mmol/L and her heart rate improved. When she had been warmed to 26⁰C, the serum
potassium corrected to 5.1 mmol/L before settling at 3.6 mmol/L (with no
potassium supplementation). Her serum phosphorous level and blood sugars normalized
when her body temperature rose above 30⁰C. She also spontaneously converted to
sinus rhythm.
This case illustrates the profound metabolic complications which
can arise in the context of extreme hypothermia. Hypokalemia is well recognized
in hypothermia, however, the drop in serum potassium levels is usually mild.
Most reported cases involve intentional body cooling in treatment of severe
head injury or post-cardiac arrest. The mechanism of hypokalemia is thought to
be redistribution of potassium back into the cell. As mentioned by Veeraish, a
case has been bravely described of a patient developing hypothermia-associated
hypokalemia while being intentionally cooled after head injury. Treatment with
potassium supplementation and re-warming occurred concurrently and the patient
then suffered a fatal arrhythmia. As the serum potassium will correct itself
with rewarming, we should be extremely cautious about administering potassium
to hypothermic patients due to the risk of severe rebound hyperkalemia.
"Core temperature 21 degrees Celsius" with K 1.1!! I am surprised she survived that! Your post does underline the profound effect of hypothermia on serum potassium, and why sometimes, not jumping to aggressively replete it might be the best approach.