To many of us IgA nephropathy (IgAN) is a disease
to be watched and monitored. Most cases of IgAN in which the clinical course is aggressive occur with
one of two atypical presentations:
to be watched and monitored. Most cases of IgAN in which the clinical course is aggressive occur with
one of two atypical presentations:
1. Acute kidney injury (AKI) and macroscopic haematuria or
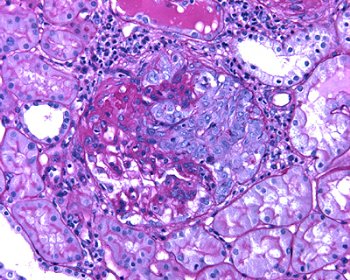
2. Nephritic syndrome or RPGN with a crescentic nephritis on biopsy
The first thing to say is that both of these
presentations are rare. Whilst visible haematuria coinciding with mucosal
infections is a well-known feature of IgAN, development of coincident acute
kidney injury is uncommon. In
fact, the largest published case series with this presentation I could find
included only 38 patients. With regards to crescentic nephritis, it
is instructive that the recently produced Oxford classification of IgAN study found so few
patients with a severe crescentic nephritis (median % gloms with crescents 9%)
that the authors were unable to include crescents as having “independent value in predicting renal outcome.”
presentations are rare. Whilst visible haematuria coinciding with mucosal
infections is a well-known feature of IgAN, development of coincident acute
kidney injury is uncommon. In
fact, the largest published case series with this presentation I could find
included only 38 patients. With regards to crescentic nephritis, it
is instructive that the recently produced Oxford classification of IgAN study found so few
patients with a severe crescentic nephritis (median % gloms with crescents 9%)
that the authors were unable to include crescents as having “independent value in predicting renal outcome.”
The
AKI seen with visible haematuria is often due to tubular injury from intra-tubular
erythrocyte casts and a possible direct nephrotoxic effect of haemoglobin. The key issue in these patients is not
so much treatment, which is through general supportive measures, but ensuring
that protracted or repeated AKI is not due to a crescentic IgAN. As a result, the recently published
KDIGO glomerulonephritis guidelines
recommend that any patients with known IgA exhibiting AKI and visible
haematuria who fail to show improvement of kidney function after 5 days should
undergo repeat renal biopsy.
AKI seen with visible haematuria is often due to tubular injury from intra-tubular
erythrocyte casts and a possible direct nephrotoxic effect of haemoglobin. The key issue in these patients is not
so much treatment, which is through general supportive measures, but ensuring
that protracted or repeated AKI is not due to a crescentic IgAN. As a result, the recently published
KDIGO glomerulonephritis guidelines
recommend that any patients with known IgA exhibiting AKI and visible
haematuria who fail to show improvement of kidney function after 5 days should
undergo repeat renal biopsy.
Crescentic
IgAN (defined as RPGN with crescents in >50% of glomeruli seen in the
biopsy) although rare has a poor prognosis: end-stage renal disease in 75% of
one cohort at 10-year follow-up. The KDIGO guidelines suggest on the
basis of low quality evidence initial treatment as for ANCA vasculitis with
steroids and cyclophosphamide.
Interestingly, no suggestion is made for maintenance therapy in these
cases.
IgAN (defined as RPGN with crescents in >50% of glomeruli seen in the
biopsy) although rare has a poor prognosis: end-stage renal disease in 75% of
one cohort at 10-year follow-up. The KDIGO guidelines suggest on the
basis of low quality evidence initial treatment as for ANCA vasculitis with
steroids and cyclophosphamide.
Interestingly, no suggestion is made for maintenance therapy in these
cases.
I
have only ever seen a single case of severe crescentic IgAN and no cases of AKI
with visible haematuria. However,
I think it’s important to know some details about these presentations. In the near future I’ll look at
Henoch-Schonlein nephritis and that most thorny of issues in IgAN; who to treat
with immunosuppression outside of an RPGN presentation.
have only ever seen a single case of severe crescentic IgAN and no cases of AKI
with visible haematuria. However,
I think it’s important to know some details about these presentations. In the near future I’ll look at
Henoch-Schonlein nephritis and that most thorny of issues in IgAN; who to treat
with immunosuppression outside of an RPGN presentation.
Hey! What happened to the piece on immunosuppression in IgA? Upcoming or what? Inquiring minds want to know.
Bob
I have a patient with HSP and 30% crescents with AKI who is HIV positive. Is there a role for plasmapheresis?
Its odd isn't it the IgA Nephropathy with crescents – most people do as you say and treat as per "crescentic Gn" and forget the IgA context. My experience of it is that is often does not respond well. Another situation you might consider in another blog/post is aggressive recurrent disease in allografts (again, histological recurrence frequent, but damage unusual). Again, response is poor in my experience.