 Creatine monohydrate is a widely available dietary supplement. It frequently pops up during both outpatient and inpatient discussions on the differential for acute kidney injury. However, the literature is scant and appears to be conflicting. So, here are a selection of some of the papers that have been published on this subject.
Creatine monohydrate is a widely available dietary supplement. It frequently pops up during both outpatient and inpatient discussions on the differential for acute kidney injury. However, the literature is scant and appears to be conflicting. So, here are a selection of some of the papers that have been published on this subject.
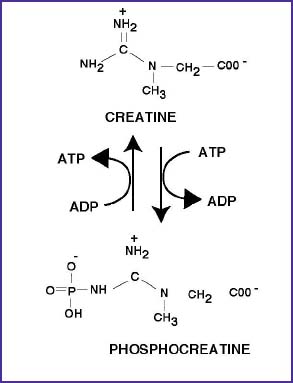
Firstly, creatine itself is produced naturally in the body, mainly by the liver and kidney, and is transported mainly to muscle. It is involved in a complex interplay with phosphate to form phosphocreatine, facilitating a stable and rapid supply of energy on demand. Creatinine (our common, but imperfect, clinical surrogate of GFR) is a breakdown product of creatine.
One of the early reports of association of exogenous creatine with kidney damage was in 1998 – the case described acute on chronic renal impairment in a 25yo man on cyclosporine for FSGS, which was temporally related to ingestion of supplemental creatine (there was no reported change in proteinuria). Upon cessation of the supplement his serum creatinine returned to baseline. No biopsy was performed.
A second case reported biopsy proven acute interstitial nephritis in a 20yo man, which occurred four days after ingestion of creatine supplements. Again, upon cessation of creatine the renal function returned to baseline.
This review of the existing literature on creatine supplements, highlights the varying reported results of the effects of exogenous creatine on both CPK and serum creatinine levels, with some claiming no change and others claiming slight elevations. An interesting randomized, double-blind, placebo-controlled trial of 18 athletes looked at the effect of creatine ingestion (10 g/day over 3 months vs placebo) on cystatin C levels as an alternative measure of eGFR. The authors claimed that creatine caused no significant alteration in estimated GFR as assessed by cystatin C (in fact the cystatin C levels decreased).
Overall, it would appear that we are still awaiting more detailed information of potential renal risk associated with exogenous creatine use. The trials to date are relatively small and longer term follow up is needed. As ever, a detailed exposure history and close vigilance is required, especially in light of the current popularity of alternative and supplement based pharmacotherapy.

@Bett, the production of creatinine as a by product of the metabolism of creatine is “neither good nor bad”, it just is what it is. The lab values showing excessive creatinine being “bad” is not accounting for creatine supplementation as used by “fitness buffs”. @Gearoid, according to this study, no conclusive evidence of impact is drawn at this time, so ceasing supplementation isn’t indicated. What may be significant is the 3 hour half life of creatine, which would indicate limited benefit to any creatine supplementation more than 4.5 hours (1/4 life) prior to exercise. Excess creatine just gets converted and urinated, potentially straining the kidneys as in the case of interstitial nephritis in the 20/m case study.
So creatinine is a breakdown product of creatine? This is good or bad?
Would you tell him to stop the creatine supplements then?
I saw a gentleman in the office – 50 years old, fanatical fitness buff (and I mean buff) who took several grams of creatine daily and was sent to me with serum creatinine of 2.9 and BUN 18. No hypertension, benign U/A, no other evidence of kidney disease. When the creatine was stopped, his creatinine want back down to 1.2. Conversion of creatine to creatinine is non-enzymatic, I suspect simply mass balance-driven. I would bet that most reported cases of "kidney damage" with creatine aren't kidney-related at all…