A 47 year old man with ESRD secondary to a chronic TMA presented 3 months following a renal transplant with a rising creatinine (1.44 mg/dl from a baseline of 0.9 mg/dl). His prograf level had ranged from 5-7. His flow XM was positive although no donor-specific antibody was detectable on a single antigen bead. His H&E stain is seen below.
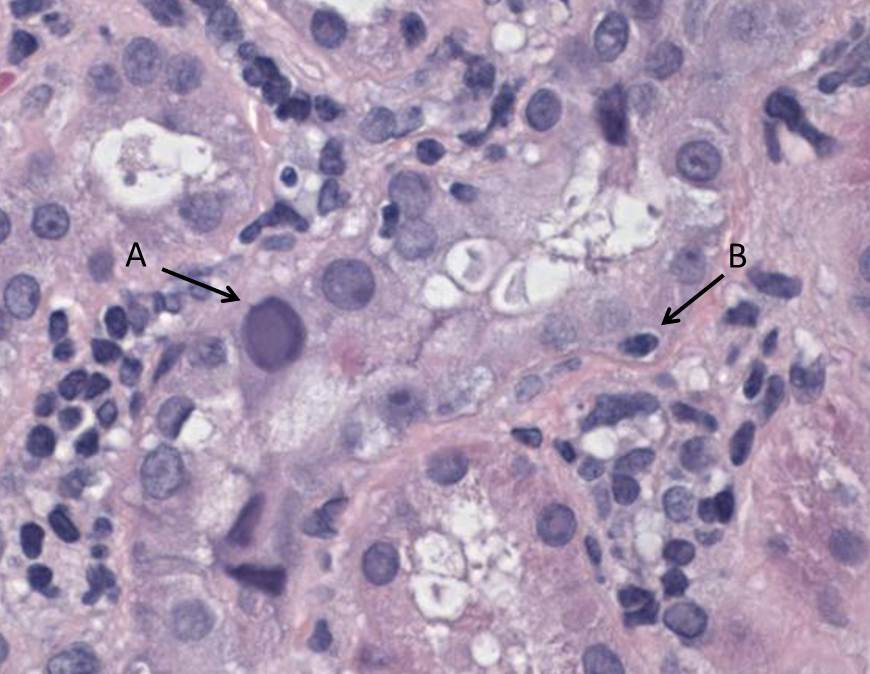
He has a moderate interstitial infiltrate. (A) marks an enlarged, abnormal nucleus with a Cowdry type B inclusion. These inclusions can be seen both in adenovirus infections and in patients with BK nephropathy. (B) marks a lymphocyte in the proximal tubular epithelium – tubulitis. The absence of significant necrosis makes adenovirus less likely and, given the recent history of a renal transplant, the likeliest diagnosis therefore is BK nephropathy.
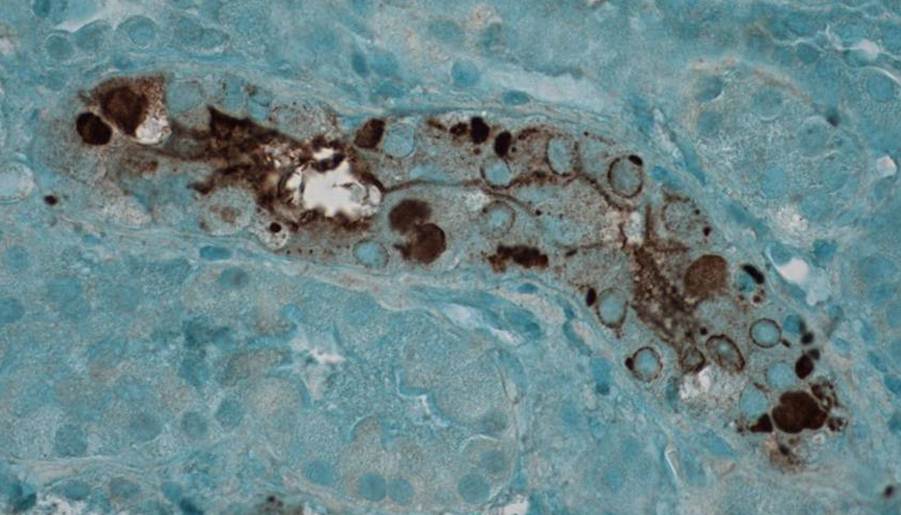
This image shows immunohistochemical staining for BK (SV-40) in the renal cortex. There is some cytoplasmic staining in surrounding tubules. However, this is non-specific. There is intense staining in the nuclei of infected cells (which are also enlarged relative to the non-infected cells) and this is highly specific for BK-virus infection.
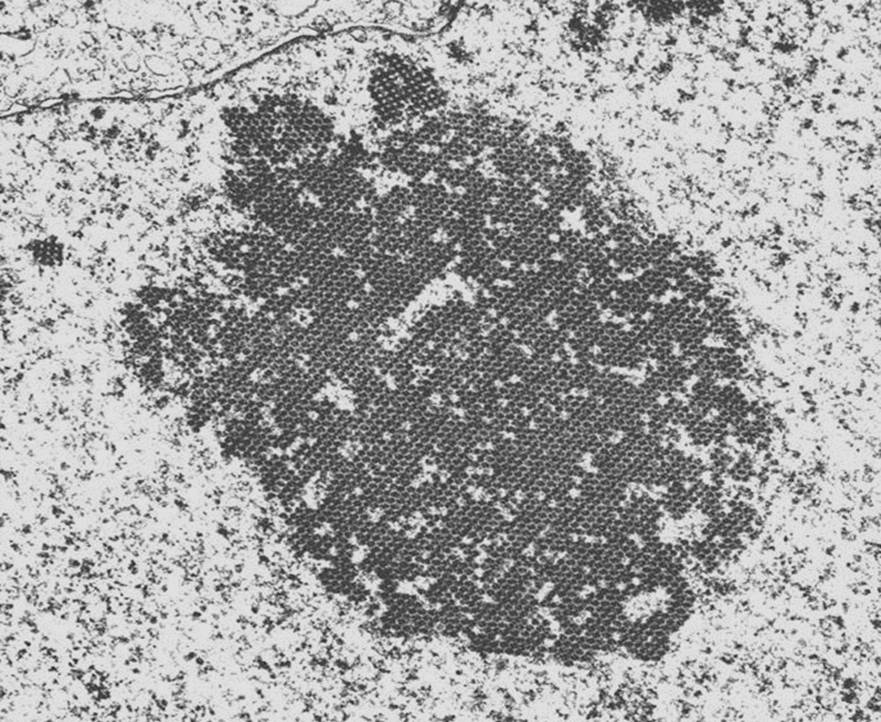
The final image is a EM image of an infected cell. Because BK-viral infection tends to be focal, it is unusual to actually see this appearance on EM. There is the appearance of a crystalline array of viral inclusions and in BK-virus, these tend to the in the range of 40-50 nm in size. In contrast, the inclusions in patients with adenovirus tend to be larger.
(Click any image to enlarge)
