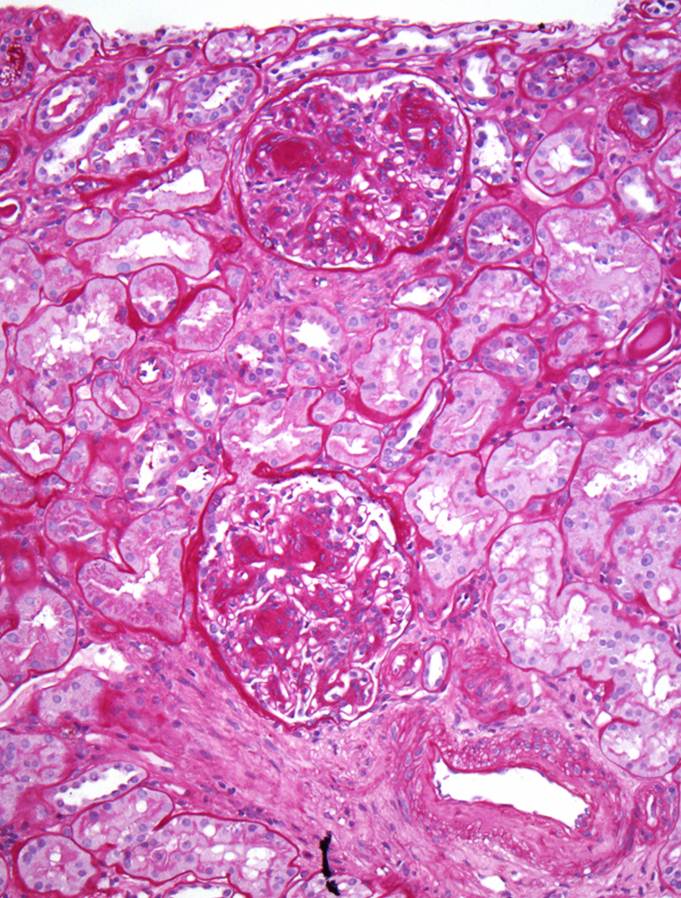
A low power view of the renal cortex revealed an obvious nodular appearance of the glomeruli. The tubules were relatively well-preserved.
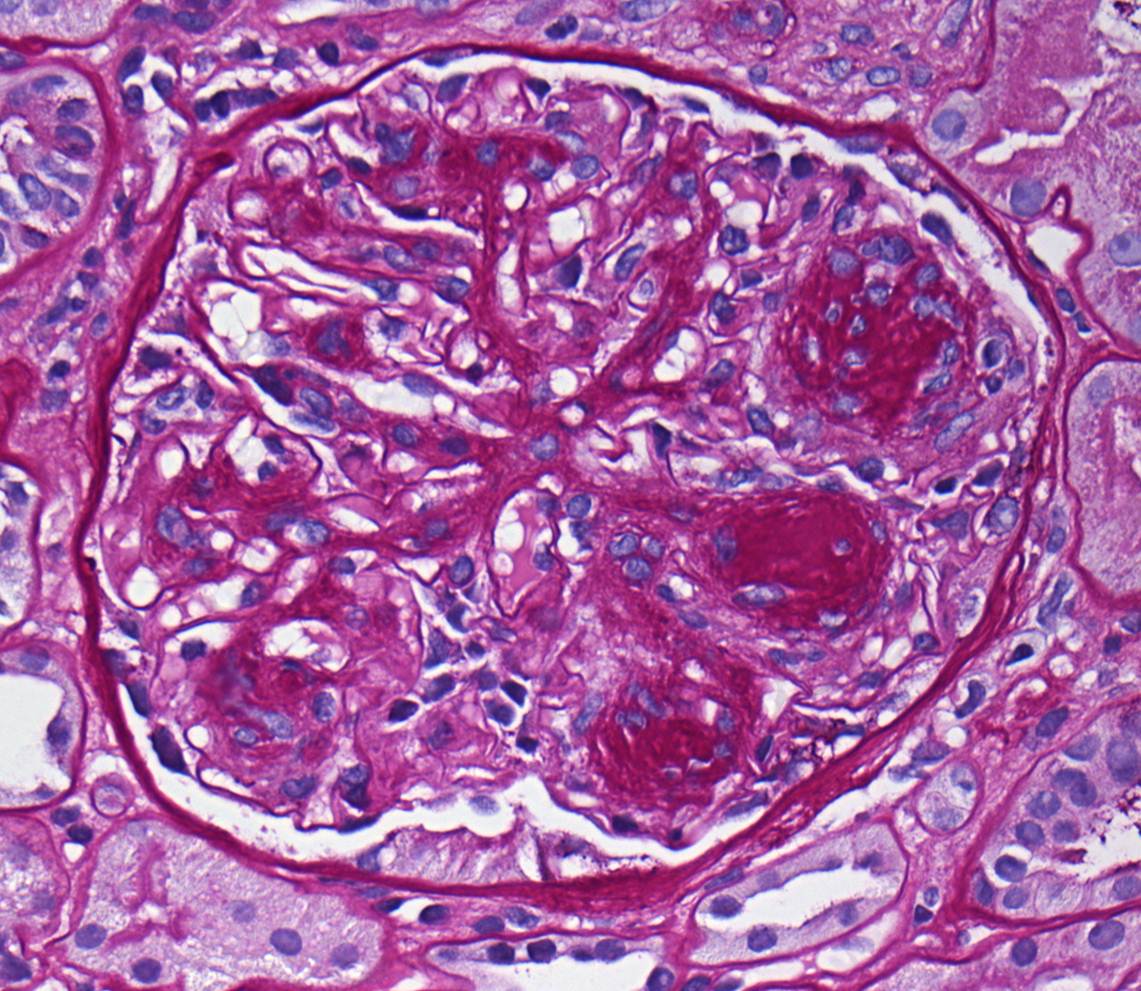
High-power view of the glomerulus was characteristic of nodular glomerulosclerosis. Notably, there was no evidence of any crescents and no thickening of the capillary loops.
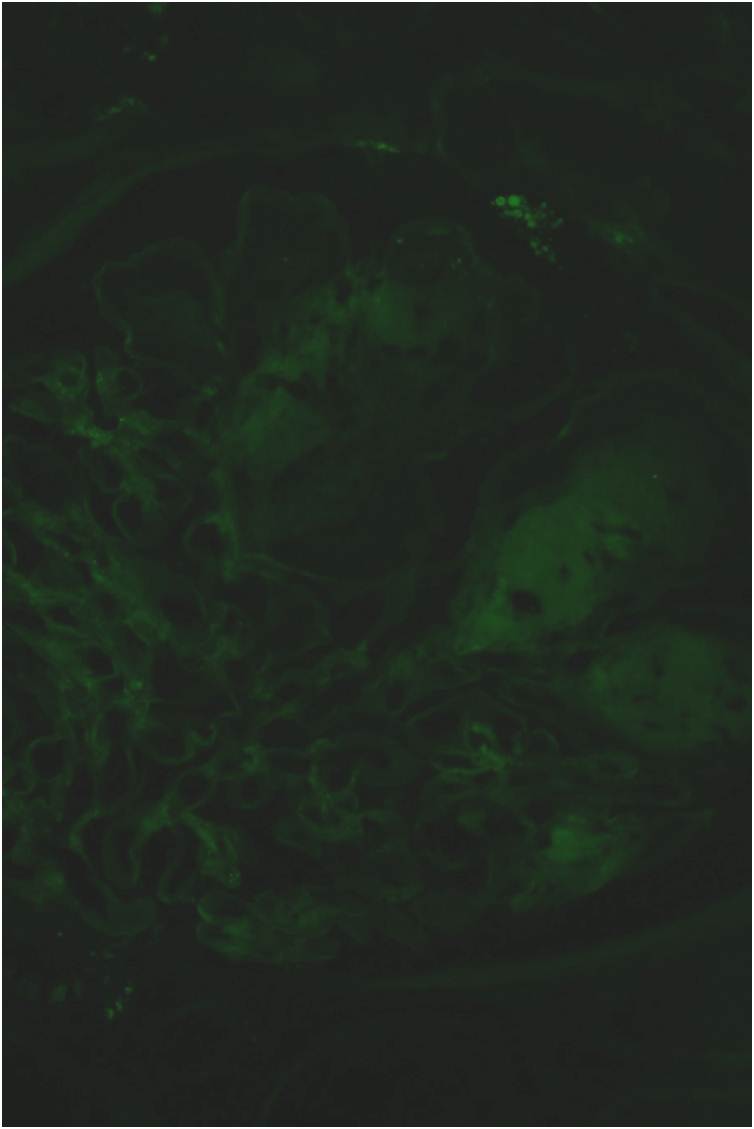
IF was completely negative
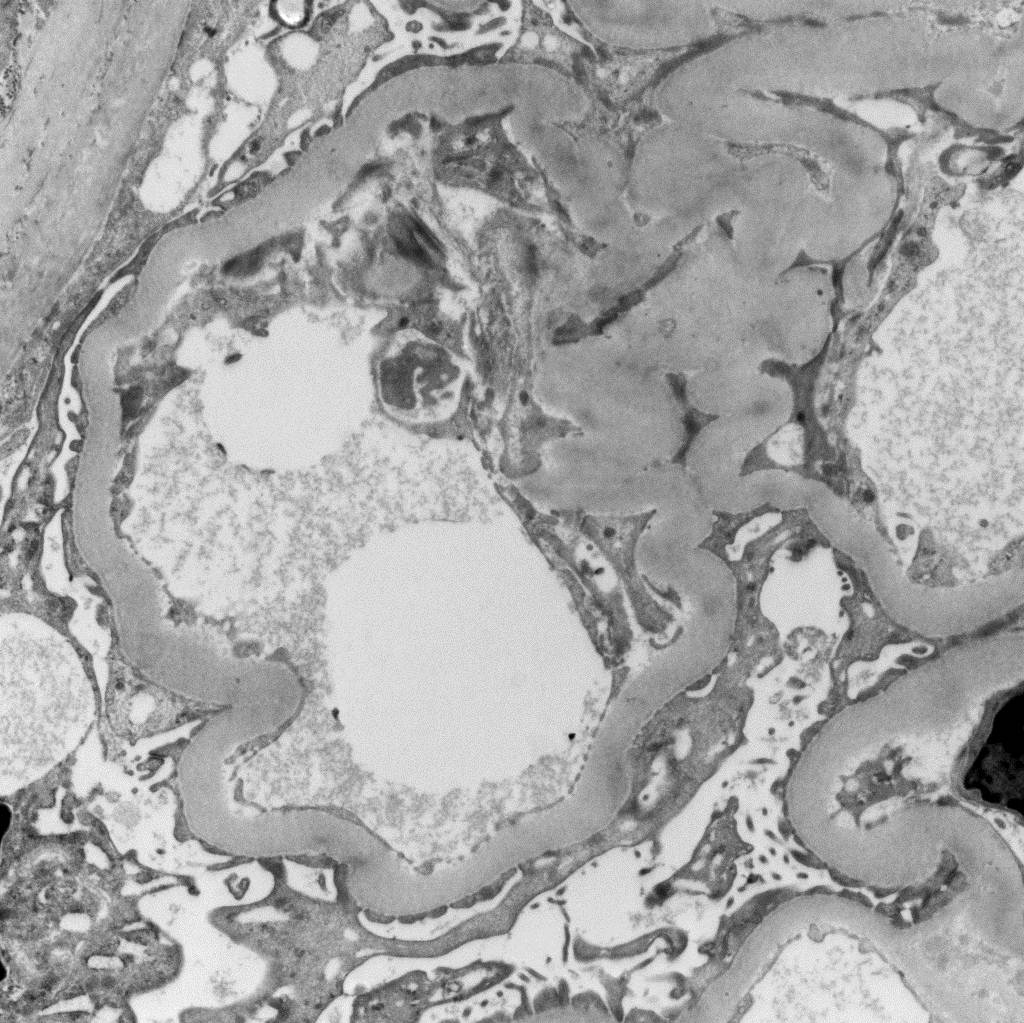
There were no medullary or BM inclusions on EM
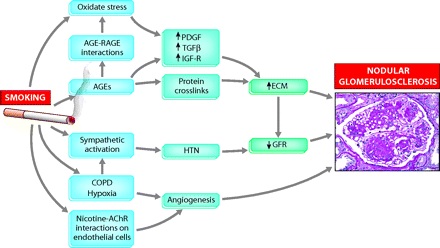
Nodular glomerulosclerosis is classically associated with diabetes and this is the first diagnosis that came to the mind of the pathologist when the slides were processed. However, the patient had no history of diabetes. Alternative diagnoses include chronic MPGN and dysproteinemias. There was no evidence of either in this case. The final diagnosis was “Idiopathic Nodular Glomerulosclerosis”. This is somewhat of a misnomer as these days, it is thought that IGN is directly related to smoking. The mechanism is uncertain but is suggested in the flow-chart below from an a review in JASN on the topic.
This is not a benign condition. In the largest case series to date of 23 patients with biopsy-proven IGN, 6 patients reached ESRD in a median of 26 months. Predictors of progression included not quitting smoking, lack of ACEi use and the degree of atrophy, fibrosis and arteriosclerosis on renal biopsy.
(Click on any image to enlarge)