An article in Annals of Internal Medicine gives us a little more information to help make an informed decision. The authors reviewed the records of 10000 patients in Ontario treated with chlorthalidone between 1993 and 2010. These were matched using a propensity score to 19000 patients treated with HCTZ and all were followed for a maximum of 5 years. All patients were over the age of 66 at the time of starting the diuretic and patients who had a major CV event in the year prior to entry into the study were excluded. The primary outcome was CV death or a major CV event. The authors believed that they were going to demonstrate a significant benefit for chlorthalidone. The overall results of the study are shown below:
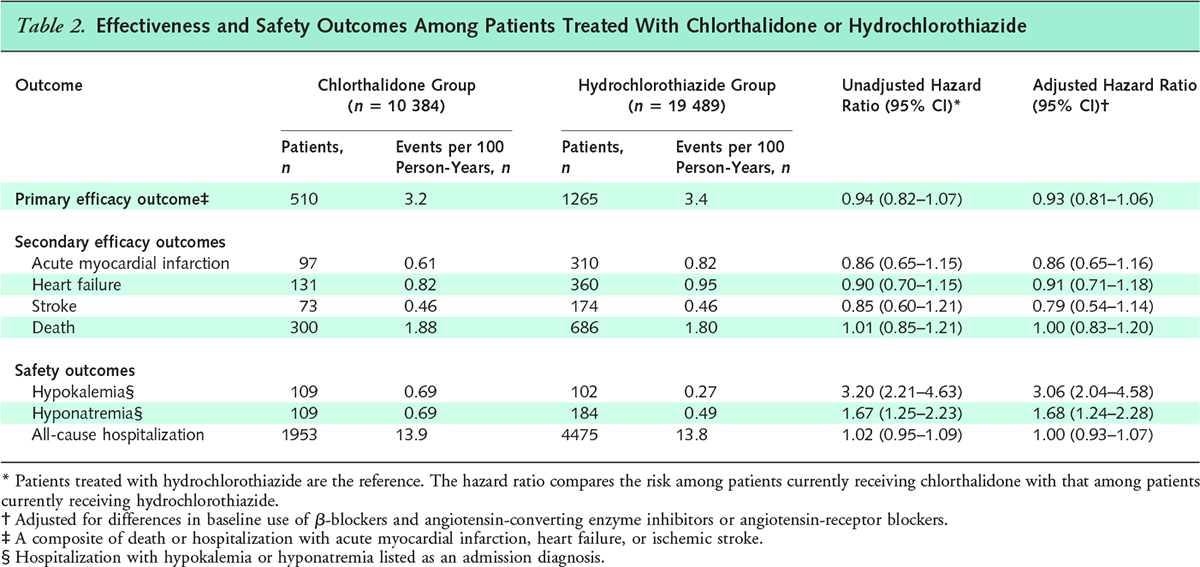
There was no difference in the primary outcome between the two groups. In a safety analysis, the use of chlorthalidone was associated with a threefold higher OR for admission with hypokalemia and almost double the OR for admission with hyponatremia. There was no difference in the risk of all-cause hospitalization. The dose of chlorthalidone available on the formulary in Canada is 50mg daily so the thought was that this difference may be related to the use of higher doses but a post-hoc analysis showed that, irrespective of the dose used, chlorthalidone was associated with a higher risk of hypokalemia and hyponatremia. Looking back, this makes sense. The half-life of chlorthalidone is so much longer than HCTZ that potassium wasting is almost guaranteed. In fact, it has been shown in the past that chlorthalidone causes potassium wasting at much lower doses than HCTZ. Technically, HCTZ should be given twice daily because of the short half-life but it generally is not. I wonder if it was, would you see the same effect on electrolyte concentrations?
There is (as always) a caveat. There may have been some unmeasured confounding. It is uncertain why some physicians may have chosen chlorthalidone over HCTZ. The other formulation of chlorthalidone that is available in Canada is a combination drug with atenolol. As a result, the rates of use of B-blockers was higher in the chlorthalidone group and the rate of the use of ACEi was lower. This is a really interesting study. I have been tending to use more chlorthalidone in my practice over the last few years based on the limited that that were available but I am not sure what the correct answer is now. It should be noted that the UK guidelines now recommend thiazides as a 3rd line therapy for hypertension following CCBs and ACEi.
This is a great interview with the first author of the paper on Medscape which is worth reading.

Exactly. There was a big difference in the use of ACEi and BB and this could have accounted for the lack of difference in outcomes. That said there were a lot more adverse effects. Remember that the bias of the authors was that chlorthalidone would be better which, in a way, makes this finding more striking.
Very interesting! I too have generally preferred chlorthalidone in my practice, though this is giving me some reason to pause.
As you point out, though, the potential confounding with the combination pill of chlorthalidone/BB is an important limitation. This is particularly true in the case of atenolol, which has been shown in a large meta-analysis (Lancet, 2005) to be independently associated with greater risk of death.