Again, we’ll break up the trials into categories:
1. Inflammation: As mentioned before, vitamin D has been shown to have anti-inflammatory effects in animal studies. A number of studies have examined the effect of vitamin D supplementation on inflammatory mediators. One study took ~120 patients with CHF and treated them with cholecalciferol or placebo for 9 months. Levels of anti-inflammatory IL-10 were higher and TNF was lower in treated patients. However, there was no difference in LVEF or mortality between the two groups and about 20% of patients did not complete even 9 months with more dropouts occurring in the vitamin D group. Similar reductions in pro-inflammatory cytokines have been noted in HD patients and patients with diabetes although these studies were too small and short-term to show any clinical effects.
2. Hypertension: Results from meta-analyses have been inconsistent with one study showing a non-significant decrease in BP with vitamin D therapy and another showing a reduction in systolic BP only. Currently, there is insufficient evidence to suggest that vitamin D is effective to treat hypertension.
3. Chronic Kidney Disease: Given the well-described relationship between vitamin D and the kidney, it is unsurprising that there has been a focus on CVD prevention in patients with CKD. Again, the results are inconsistent with some studies showing a benefit in terms of CV risk and others being negative. The PRIMO study examined LV mass index in patients with CKD and looked at the effect of 48 weeks treatment with activated vitamin D. There was no difference in the primary outcome among the two groups. One important point is that, in the past, there was no focus on 25OH vitamin D in patients with CKD due to the perception that it is biologically inactive. This perception is changing and there may be a role for increased 25OH vitamin D supplementation in CKD patients although this role has not yet been fully defined.
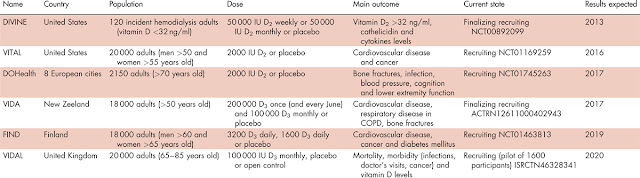
4. Cardiovascular Death and stroke: Large meta-analyses have suggested a benefit of vitamin D therapy on all-cause mortality. The results for CV mortality and morbidity are less consistent although a benefit has been shown in some trials. One issue is that most studies do not limit treatment to patients with vitamin D deficiency while subgroup analysis of some trials shows that there is more benefit of therapy in these patients. There are a number of large trials of vitamin D currently ongoing (see table below from this recent review). Hopefully we will be able to get a clearer picture of the benefits of vitamin D therapy in the near future.
Overall, the results of the intervention trials have been disappointing and inconsistent – particularly given the strength of the observational and experimental data. At this point, we still don’t know the exact role for vitamin D in the prevention and management of CV disease. There is always the suspicion that unmeasured confounders have an important part to play. The best way to get an answer is by doing well-designed RCTs and perhaps when these ongoing trials are complete, we will have a fuller idea of this role.
