
The advent of SGLT2 inhibitors has allowed us to test this theory in both animal models and humans. Recently, a small physiologic study was published in Circulation which tested the effect of SGLT2 inhibition in individuals with type 1 DM stratified by the presence or absence of hyperfiltration at baseline. GFR was measured using inulin clearance. The figure above is taken from the paper and shows the putative mechanism for hyperfiltration and the role of SGLT2 inhibitors. In this paper. empaglifozin treatment for 8 weeks lead to a significant decrease in weight, BMI, daily insulin dose and carbohydrate intake in both groups. In the normofiltration group, it had no effect on renal hemodynamics. However, in the hyperfiltration group, there was a significant reduction in GFR (-33ml/min), renal plasma flow, renal blood flow and an increase in renal vascular resistance. These results are remarkable but to me it does beg a question.Why is there such a dramatic effect in the hyperfiltration patients and what makes them different in the first place. Based on the evidence of this study, most of the hyperfiltration is indeed related to increased TGF. Looking at table 1 gives a hint of what might be the correct answer.
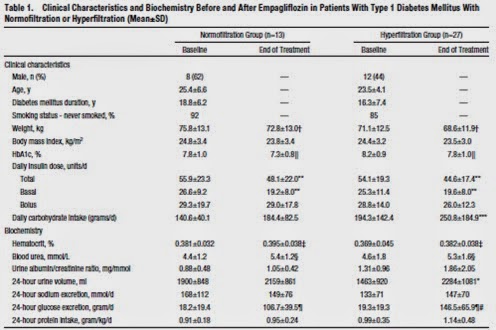
The baseline BMI and insulin doses were similar in both groups. However, the HbA1c was marginally higher in the hyperfiltration group as was the baseline carbohydrate intake. 24 hour glucose excretion was identical in the two groups. Following treatment, the daily carbohydrate intake increased significantly in both groups but to approximately the same extent. However, the increase in 24 hour urine glucose was substantially higher in the hyperfiltration group. What this suggests to me is that the hyperfiltration may be driven by higher overall carbohydrate intake despite relatively similar HbA1c levels. Because the 24 hour glucose excretion was the same in both groups prior to treatment, this suggests that the majority of the filtered glucose was being reabsorbed. Because the hyperfiltration group were taking in more carbohydrate, this would lead to an increase in the delivered load of glucose to the proximal tubule with a consequent increase in NaCl reabsorption. Treatment with empaglifozin prevented the kidneys from reabsorbing this excess glucose and this is reflected in the fact that the 24 hour urine glucose increased more in the hyperfiltration group than the normofiltration group.
I should point out that this is my theory alone based on the reading of this paper and that many of these between group differences were not statistically significant because of the low numbers of patients involved. Still, this paper at least provides elegant proof of the role of proximal glucose reabsorption on the maintenance of hyperfiltration.
