 For my inaugural RFN post, a special case I saw last year with Dr. David Mount and Young-Soo Song a fellow nephrologist in training at BMC.
For my inaugural RFN post, a special case I saw last year with Dr. David Mount and Young-Soo Song a fellow nephrologist in training at BMC.
A 74-year-old man with history of HTN, peripheral artery disease, CKD (baseline Cr 1.6) who initially presented with NSTEMI. He was placed with a balloon pump (IABP), and underwent CABG on Day 2. Post-operatively he was quickly weaned off pressors. On Day 3, the IABP was removed. He suddenly became anuric. His creatinine increased from 2.0 on Day 2 to 3.17.
He was evaluated for the differential of anuric AKI, we had a high suspicion for renal artery occlusion, due to the relation to the retrieval of the IABP. Angiography confirmed complete occlusion of the renal arteries. Attempts at IR-thrombectomy failed, the renal arteries were bluntly occluded at the level of the aorta.
We decided to pursue revascularization despite some doubts from surgery. He underwent a Hepato-right renal artery bypass on day 7 (4 days after the insult). He was off dialysis, urinating freely with decreasing creatinine in less than a week.
Clues that revascularization was going to be successful:
– On renal ultrasound the right kidney was 10.8 cm with normal echotexture. But the left kidney was 8.79 cm with cortical thinning suggesting a chronic renovascular disease.
– The MAG-3 scan showed persistent perfusion of the right kidney
From experimental models of renal ischemia, we know that there’s irrevocable destruction of the kidney, within hours of loss of perfusion (Sanchez Fructuoso, JASN 2000; Hamilton PB, Am J Physiol. 1948). However, there’s a minimal perfusion pressure that is capable of maintaining nephron viability without sustaining filtration (Moyer, Annals Surg 1957).
From experimental models of renal ischemia, we know that there’s irrevocable destruction of the kidney, within hours of loss of perfusion (Sanchez Fructuoso, JASN 2000; Hamilton PB, Am J Physiol. 1948). However, there’s a minimal perfusion pressure that is capable of maintaining nephron viability without sustaining filtration (Moyer, Annals Surg 1957).
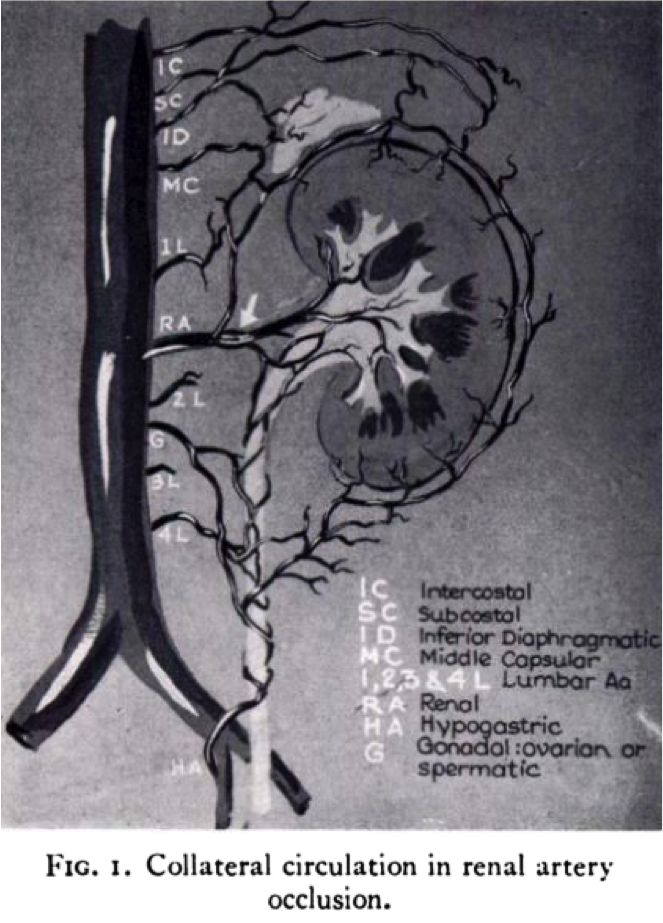
Renal perfusion is not only via the renal artery. There are small preformed collaterals that originate from the lumbar, internal iliac, gonadal, adrenal, renal capsular, intercostal, and mesenteric arteries. They can drain into the distal part of the renal artery or provide direct cortical perfusion (Love L, et al. Am J Roentgen 1968 and Lohse JR, Archives of Surgery 1982). Renal ischemia provides a maximal stimulus for vasodilatation of these collaterals.
In the case of our patient, his right kidney likely had sub-clinical renovascular disease that led to development of these collaterals. On occlusion of the renal artery he had sufficient collateral perfusion to maintain enough nephron viability to get off dialysis.
In this table are a few examples that show how long these collaterals can maintain viability.
|
Time To
revascularization |
Injury
|
Citation
|
|
6 days
|
Endovascular
aneurysm repair |
|
|
3 months
on HD |
Atherosclerotic
|
|
|
6 months
on HD |
Occlusion
of solitary kidney artery graft |
As per Dr. Cohen and Townsend’s discussion in 2001, proposed criteria to consider revascularization of the renal artery include:
-Patent distal main renal artery or the identification of collaterals. It’s important to notify the interventionalist that we’re looking for that, a routine angio will not pick that up easily.
-Biopsy evidence of viable glomeruli in a representative specimen.
-Renal size greater than 9 cm
-Evidence of perfusion either by MAG-3 scan (debatable) or Renal Doppler
Charbel C. Khoury


Hi Neil,
it’s Love L, Bush I M, American Journal of Roenterology 1968
Please find pdf https://drive.google.com/file/d/1_oBuNe_81qgzHV7bzoRikFcG2D0mqtTv/view?usp=drivesdk
Hope this helps
Great report, and figure (fig 1) – could you cite source?