Azathioprine is one of the oldest immunosuppressant medications, which has been used in the field of solid organ transplantation over the past 5 decades. It is metabolized into its inactive forms by the enzyme thiopurine methyltransferease (TPMT). Genetic polymorphisms of the gene coding for this enzyme are common in the general population (~ 10% are heterozygotes causing low enzyme activity and ~ 0.3% cause complete lack enzyme activity). Testing for the enzyme activity is recommended prior to treatment with azathioprine or any thiopurines in children. However, it is not consistently tested for in adult patients who are immunosuppressed with azathioprine for inflammatory bowel disease, organ transplantation or rheumatologic conditions.
Genotypic (testing for polymorphisms in the TPMT gene) and phenotypic (measuring levels of substrates and products of the enzyme in RBCs) testing for TPMT are commercially available but the concordance between them is not 100%.
The following are the metabolites that are tested for in the phenotypic testing:
6- Mercaptopurine – (Ref: 3.0- 6.6) nmol/ml/hr
6- Methylmercaptopurine riboside – (Ref: 5.04 – 9.57) nmol/ml/hr
6- Methylthioguanine riboside – (Ref: 2.7 – 5.8) nmol/ml/hr
Phenotypic testing performed within 30-90 days after a blood transfusion can result in inaccurate interpretation of the results because of donor RBCs influencing the test results. Moreover ethnicity, type of disease, concurrent drug treatment, red cell kinetics and transfusions should be taken into account while interpreting the results of TPMT enzyme activity. Single nucleotide polymorphisms (SNPs) account for the major TPMT low activity variant forms. Four TPMT alleles, TPMT*2, *3A, *3B, and *3C, account for over 90% of inactivating polymorphisms.

The approximate commercial cost is ~ $200 for phenotyping and ~$450 for genotyping.
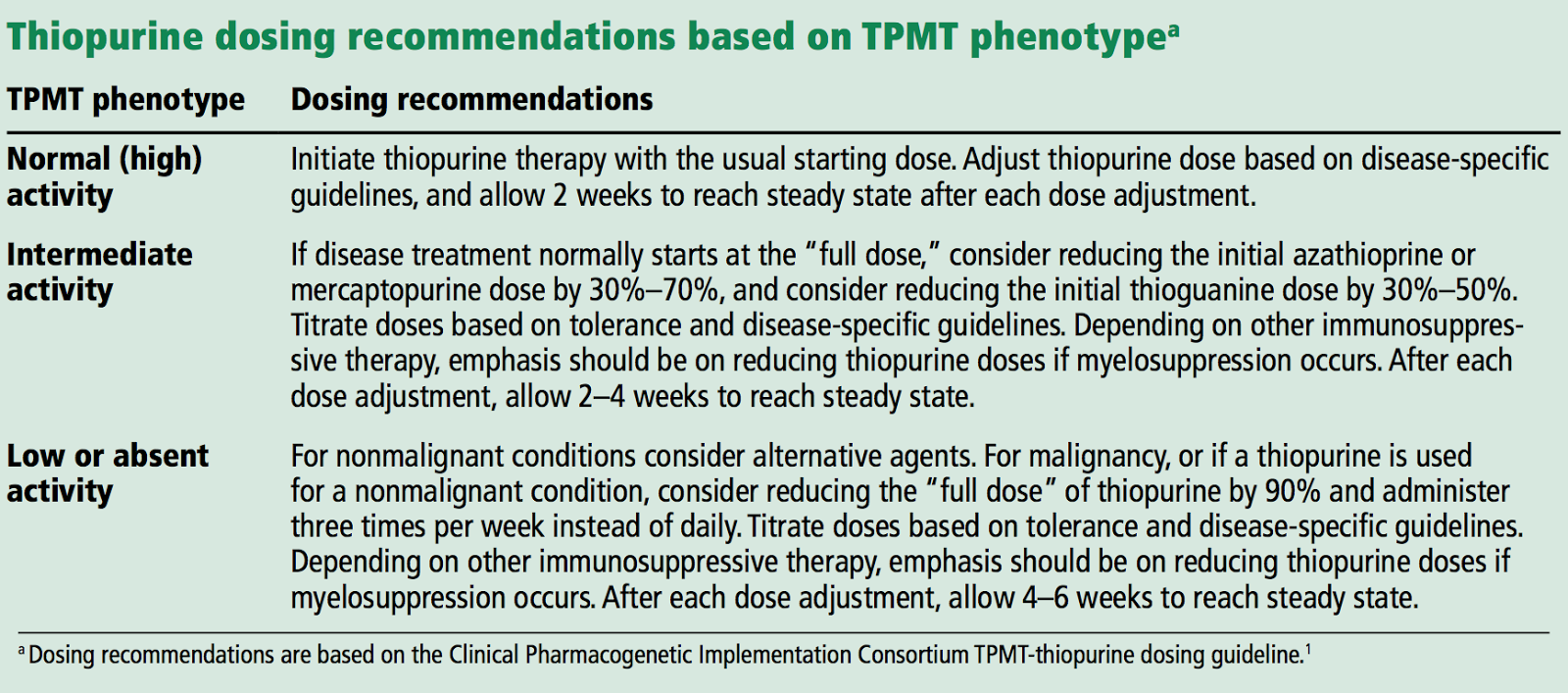
Clinical Pharmacogenetic Implementation Consortium (CPIC) has developed an evidence-based guideline on how to adjust thiopurine doses based on TPMT activity.
Posted by Karthikeyan Venkatachalam
Transplant Fellow
Washington University School of Medicine
St Louis

Hi Karthikeyan,
Interesting to read about Aza toxicity. We have see a similar interaction between Aza and Febuxostat resulting in severe bone marrow suppression( lethal at times with hemoglobin dropping to as low as 3g within a span of 2 weeks). The combination of Aza and Allopurinol is not recommended in view of this interaction. The same applies to Febuxostat as well. But this is not well stressed in the guidelines. Since Febuxostat is a safe drug otherwise, we tend to prescribe it instantaneously in hyperuricemic patients. The newly joined residents often make this mistake.
Anand Chellappan
Nephrology Senior resident
SGPGI, India