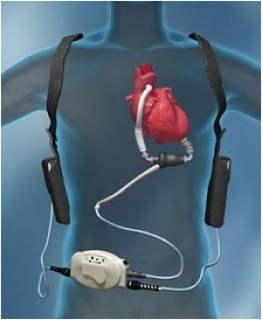
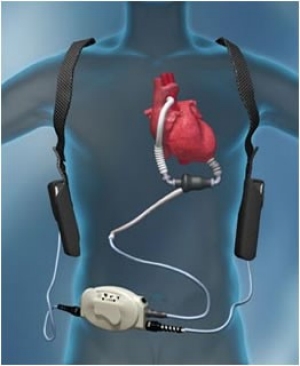
This is part 2 of a blog
on LVAD for the nephrologist. Part 1 may be found here.
on LVAD for the nephrologist. Part 1 may be found here.
Predicting reversibility
of renal dysfunction is a difficult task in the setting of heart disease and has
a significant effect on patient prognosis. Patients with low GFR may have their
kidney function improved after LVAD implantation due to an increase in kidney perfusion. Or it may continue to be poor due to pre-existing intrinsic kidney disease.
of renal dysfunction is a difficult task in the setting of heart disease and has
a significant effect on patient prognosis. Patients with low GFR may have their
kidney function improved after LVAD implantation due to an increase in kidney perfusion. Or it may continue to be poor due to pre-existing intrinsic kidney disease.
- Some studies show that
patients with low GFR prior to LVAD had initial improvement in creatinine but a
gradual decline in GFR over the next several months. Despite this, GFR at one
year was still more than the pre-LVAD level. Interestingly patients with normal
pre-LVAD GFR had a small but steady decline in kidney function after the
implantation. Probable reasons for the late decline in kidney function could due
to a measurement bias (less muscle mass at the time of LVAD surgery, so low
creatinine levels post LVAD, muscle mass improves with
rise in creatinine), hemolysis or RV dysfunction (seen in up to 10 % patients post–LVAD). - Another unique possibility is an effect of continuous flow physiology
on renal vessel walls (animal studies show arterial smooth muscle hyperplasia, periarteritis
and interstitial inflammation & fibrosis; no human data). Bresco et al, demonstrated
an unexpected survival analysis based on GFR change in first month of LVAD
implantation. They showed that patients who had greater than 88 % rise in GFR within one
month had a poor survival rate, followed by patients with any degree of
worsening of kidney function after LVAD implantation. The best survival was in
patients with modest GFR improvement (22-47%). One possible explanation for
this could be that patients who are severely ill prior to LVAD are likely to be
those with worse kidney function. Could they then have a larger improvement in kidney perfusion and therefore kidney function, in the early post
LVAD period?
 Dialysis Post LVAD:
Dialysis Post LVAD:
The incidence of AKI varies between studies, ranging from 7 to 56%, possibly due to different definitions of AKI, severity of underlying of cardiac & kidney disease, and has an adverse impact on patient survival post-LVAD. Patient with AKI also have poor bridge to transplantation rates (52.4 %vs 83.5 %).
LVAD implantation in the ESRD
population has an even worse prognosis, with one recent study
describing a mortality rate of 81.9 % compared to 36.4 % in a non-ESRD group
after a median follow up of over 2 years. Does this preclude patients with advanced
renal failure from LVAD implantation? Combined heart-kidney transplantation may
be a viable option for some, and for those who do not have recovery of kidney function after LVAD-associated AKI.
population has an even worse prognosis, with one recent study
describing a mortality rate of 81.9 % compared to 36.4 % in a non-ESRD group
after a median follow up of over 2 years. Does this preclude patients with advanced
renal failure from LVAD implantation? Combined heart-kidney transplantation may
be a viable option for some, and for those who do not have recovery of kidney function after LVAD-associated AKI.
Dialysis options in
patients with LVAD include HD & PD. There are no head to head trials
comparing the two. PD appears more attractive in my view as it offers more
gentle ultrafiltration, less risk of systemic infections and it`s a home
modality which keeps the infection prone LVAD patients away from hospital. Very
few case reports of
PD in LVAD have been published which described successful dialysis in these
patients. A couple of practical aspects about PD in this setting:
patients with LVAD include HD & PD. There are no head to head trials
comparing the two. PD appears more attractive in my view as it offers more
gentle ultrafiltration, less risk of systemic infections and it`s a home
modality which keeps the infection prone LVAD patients away from hospital. Very
few case reports of
PD in LVAD have been published which described successful dialysis in these
patients. A couple of practical aspects about PD in this setting:
- imaging of the abdomen should
be done prior to PD catheter insertion to confirm that no element of LVAD is
intra peritoneal - PD catheter exit site should be far away from the drive
line exit site.
HD is the most frequently
used dialysis modality in this population.
There are case reports of all forms of HD done in these patients-regular
HD, CRRT and even home HD. Access is an important issue to be discussed.
used dialysis modality in this population.
There are case reports of all forms of HD done in these patients-regular
HD, CRRT and even home HD. Access is an important issue to be discussed.
- For catheter
insertion, we need to remember not to reverse the anticoagulation in these
patients. The person doing the cannulation should be trained to do the
intervention in a fully anticoagulated individual. It’s always prudent to use
fluoroscopy for these procedures as it reduces the risk of complications, like
a guide wire inadvertently damaging the VAD pump. It’s important to perform the
procedure under aseptic conditions and avoid bedside procedures. Tunneled
catheters are preferred in this regard as they are associated with less risk of
infections. If we are forced to do the cannulation without fluoroscopy
guidance, it`s preferable to use a short guide wire (10-12 cm). - Long term access should be
a fistula or graft if possible. There are no direct studies comparing these 2 accesses.
While the initial preference was for graft due to concerns of poor fistula
maturation with the continuous flow, there are published
cases of patients who had successful fistula creation while on LVAD. Of the
6 cases described, 2 of them required
balloon assisted maturation and the other 4
had unassisted maturation which were successfully cannulated. The more
difficult aspect of long term access is a thrill or bruit cannot be appreciated
in these patients. The only way of assessing patency of the access is with the
help of Doppler or direct cannulation. - Very few case series of
patients on HD have been described. One of them
included 10 patients who underwent 281 sessions of HD after post-LVAD AKI. 15
of these sessions were interrupted with symptomatic hypotension being the
reason in 6 instances (3 catheter related blood stream infections; 3 volume
related). - Dialysis centres accepting
patients on LVAD for HD should have their nurses and doctors trained to
interpret the basic LVAD parameters and make necessary changes to hemodialysis
prescription accordingly. Specifics about BP measurement were described in part
1 of this post.
The increasing number of patients with LVADs
definitely poses a challenge to the Nephrologist. Learning about the
device parameters and monitoring is fast becoming essential for us to manage these
patients. More research is warranted to understand the implications of this extraordinary
treatment for renal function and provision of renal replacement therapy.
definitely poses a challenge to the Nephrologist. Learning about the
device parameters and monitoring is fast becoming essential for us to manage these
patients. More research is warranted to understand the implications of this extraordinary
treatment for renal function and provision of renal replacement therapy.
Post by Sriram Sriperumbuduri

