Advanced heart
failure is associated with very poor survival rates of about 10 % at one year.
Treatment options include cardiac transplantation or cardiac assist devices. A
left ventricular assist device (LVAD) is a mechanical circulatory support for
patients with advanced heart failure. Previously considered only as a bridge to
transplant, these are becoming more common as a ‘destination’, and used in
patients with end stage heart disease patients who are not heart transplant
candidates. Of interest to us, this poor cardiac function in heart failure is often
complicated by renal dysfunction, the so-called ‘cardio-renal
syndrome’. This blog focuses on the outcomes of renal dysfunction in
patients with LVAD and few aspects of renal replacement therapy (RRT) in them.
I would discuss this in 2 parts to facilitate coverage of all aspects.
failure is associated with very poor survival rates of about 10 % at one year.
Treatment options include cardiac transplantation or cardiac assist devices. A
left ventricular assist device (LVAD) is a mechanical circulatory support for
patients with advanced heart failure. Previously considered only as a bridge to
transplant, these are becoming more common as a ‘destination’, and used in
patients with end stage heart disease patients who are not heart transplant
candidates. Of interest to us, this poor cardiac function in heart failure is often
complicated by renal dysfunction, the so-called ‘cardio-renal
syndrome’. This blog focuses on the outcomes of renal dysfunction in
patients with LVAD and few aspects of renal replacement therapy (RRT) in them.
I would discuss this in 2 parts to facilitate coverage of all aspects.
I will start
with few basics of LVAD that helps in understanding the intricacies of
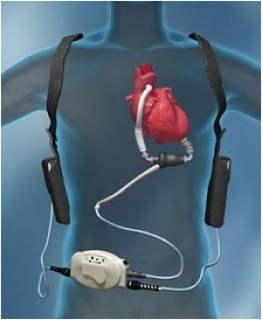
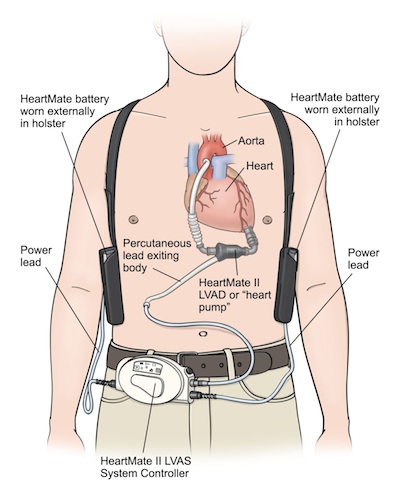
monitoring in HD patients. LVAD consists of an inflow cannula that connects to the
left ventricular apex and outflow cannula that connects to the aorta, ascending
or descending. A pump connects these two cannulas. An external device, a system
controller displays all the LVAD parameters and helps in adjusting the device
settings. The pump connects to the controller via a drive-line/percutaneous lead
that tunnels subcutaneously and exits the abdominal wall. The power supply is through
two batteries that are worn by the patient all the time with adequate backups
at their disposal, just in case (see image).
with few basics of LVAD that helps in understanding the intricacies of
monitoring in HD patients. LVAD consists of an inflow cannula that connects to the
left ventricular apex and outflow cannula that connects to the aorta, ascending
or descending. A pump connects these two cannulas. An external device, a system
controller displays all the LVAD parameters and helps in adjusting the device
settings. The pump connects to the controller via a drive-line/percutaneous lead
that tunnels subcutaneously and exits the abdominal wall. The power supply is through
two batteries that are worn by the patient all the time with adequate backups
at their disposal, just in case (see image).
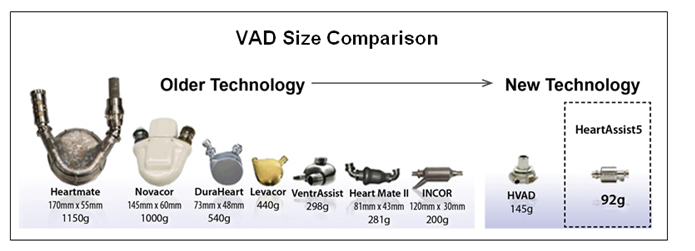
The anatomy and
physiology of LVAD has changed over decades (see image below), from a pulsatile
flow(pf)-LVAD which were big and relied on pneumatic compression system to pull
in and out blood through vascular system to continuous flow(Cf)-LVAD which are
more compact and use a power operated rotatory element for moving the blood.
The complex structure, large size and the decreased durability were mainly
responsible for pushing the pf-LVAD from the main stream and making them
obsolete. They were frequently placed in the peritoneal cavity and patients
were quite troubled from the noise produced by this device.
physiology of LVAD has changed over decades (see image below), from a pulsatile
flow(pf)-LVAD which were big and relied on pneumatic compression system to pull
in and out blood through vascular system to continuous flow(Cf)-LVAD which are
more compact and use a power operated rotatory element for moving the blood.
The complex structure, large size and the decreased durability were mainly
responsible for pushing the pf-LVAD from the main stream and making them
obsolete. They were frequently placed in the peritoneal cavity and patients
were quite troubled from the noise produced by this device.
A Cf-LVAD is
much smaller and does not have the complex structure associated with its
predecessor. They are more durable and are usually placed in the abdominal wall
(e.g. Heartmate 2) or in the pericardial space (e.g. Heartmate 3 or
HVAD/Heartware). Two subtypes of Cf-LVAD exist depending on the type of
rotatory pump. The axial flow pump rotates like a propeller in a pipe where in
blood flows parallel to the pump and the centrifugal flow pump is a spinning
disk with blades with outflow of blood tangential to the disk. Heartmate 2 and
Heartmate 3/HVAD are examples of axial flow & centrifugal flow devices
respectively.
much smaller and does not have the complex structure associated with its
predecessor. They are more durable and are usually placed in the abdominal wall
(e.g. Heartmate 2) or in the pericardial space (e.g. Heartmate 3 or
HVAD/Heartware). Two subtypes of Cf-LVAD exist depending on the type of
rotatory pump. The axial flow pump rotates like a propeller in a pipe where in
blood flows parallel to the pump and the centrifugal flow pump is a spinning
disk with blades with outflow of blood tangential to the disk. Heartmate 2 and
Heartmate 3/HVAD are examples of axial flow & centrifugal flow devices
respectively.
A few points
about LVAD parameters at this stage:
about LVAD parameters at this stage:
1) Pump speed–
the only parameter in the LVAD that can be adjusted and directly influences the
pump flow. Very high pump speeds may have consequences such a) hemolysis and
platelet activation (due to shear stress on cells), b) supravalvular thrombosis
(Cf-LVAD increase diastolic blood pressure -> decreases
trans-aortic valve pressure gradient -> decreases
frequency and duration of AV valve opening -> decreases blood flow through AV valve -> stasis of
blood in the supravalvular region -> thrombosis),
c) Right ventricular (RV) dysfunction (increased LVAD flow -> more unloading of left heart -> left
shift of interventricular septum (IVS) -> increased RV
cavity size -> impaired mechanics of RV contraction + pull over septal leaflet of
tricuspid valve with regurgitation -> RV failure)
and in extreme cases can lead to d) suction event (very high flow rates -> increased unloading of LV -> collapse of
LV on the inflow cannula), which can be fatal as it decreases the outflow and
causes arrthymia (IVS impinges on the cannula).
the only parameter in the LVAD that can be adjusted and directly influences the
pump flow. Very high pump speeds may have consequences such a) hemolysis and
platelet activation (due to shear stress on cells), b) supravalvular thrombosis
(Cf-LVAD increase diastolic blood pressure -> decreases
trans-aortic valve pressure gradient -> decreases
frequency and duration of AV valve opening -> decreases blood flow through AV valve -> stasis of
blood in the supravalvular region -> thrombosis),
c) Right ventricular (RV) dysfunction (increased LVAD flow -> more unloading of left heart -> left
shift of interventricular septum (IVS) -> increased RV
cavity size -> impaired mechanics of RV contraction + pull over septal leaflet of
tricuspid valve with regurgitation -> RV failure)
and in extreme cases can lead to d) suction event (very high flow rates -> increased unloading of LV -> collapse of
LV on the inflow cannula), which can be fatal as it decreases the outflow and
causes arrthymia (IVS impinges on the cannula).
2) Pump flow
– defines the amount of blood flowing through the LVAD pump in a minute. It can
be as high as 10 L/minute. It is directly proportional to the pump speed and
inversely to the head pressure (defined as pressure difference between the LV
cavity and the aorta). A decrease in preload due to vasodilatation
(drugs/sepsis) can increase the flow rate. On the contrary, hypovolemia (e.g.
more ultrafiltration in dialysis), RV dysfunction, and tamponade decrease
preload and subsequently the flow. Hypertension by increasing the afterload has
a similar effect.
– defines the amount of blood flowing through the LVAD pump in a minute. It can
be as high as 10 L/minute. It is directly proportional to the pump speed and
inversely to the head pressure (defined as pressure difference between the LV
cavity and the aorta). A decrease in preload due to vasodilatation
(drugs/sepsis) can increase the flow rate. On the contrary, hypovolemia (e.g.
more ultrafiltration in dialysis), RV dysfunction, and tamponade decrease
preload and subsequently the flow. Hypertension by increasing the afterload has
a similar effect.
3) Pulsatility
Index (PI) –a dimensionless variable which reflects the contractility of LV
and it varies directly according to underlying LV function with low PI
indicating worsening of LV function due to either a decrease in preload (again
can happen in dialysis) or progression of underlying heart disease or an effect
of negative inotropes on the right heart. During dialysis, it`s safe to
maintain the PI.
Index (PI) –a dimensionless variable which reflects the contractility of LV
and it varies directly according to underlying LV function with low PI
indicating worsening of LV function due to either a decrease in preload (again
can happen in dialysis) or progression of underlying heart disease or an effect
of negative inotropes on the right heart. During dialysis, it`s safe to
maintain the PI.
 How to monitor
How to monitorpulse and blood pressure in patients on LVAD? Well it`s tricky, as Cf-LVAD has
a continuous flow physiology. So the pulse is not felt in more than half of
these patients. Definitely scary to see a living person with no palpable pulse!
The presence or absence of pulse depends on underlying LV function. And it`s
even more difficult to monitor blood pressure. If patient has a radial pulse,
we can measure pressure manually or with an automated machine. If pressures
cannot be obtained with this, a Terumo device could be used for recording. This
device has 2 cuffs- large & small which are more sensitive for low pulse
pressure and hypovolemia. If radial pulse is not felt, then the best way to
measure blood pressure is with the help of a Doppler. The cuff is tied over the
upper arm and brachial artery is localized with Doppler. The cuff is inflated until
the Doppler signal is lost. On slow deflation, the pressure at which the first
Doppler signal is heard corresponds to the mean arterial pressure (MAP). So in
patients with LVAD, we have essentially only one pressure recording, MAP of `x`
mm Hg. It`s always advisable to maintain MAP between 70-80 mmHg. High MAP (especially greater than 90
mmHg) is associated with decrease in blood flow through the pump and
thrombosis.
ACE inhibitors
or ARBs are the drug of choice for hypertension control in these patients.
Vasodilators are frequently used if MAP is very high. Negative inotropes especially
non dihydropyridine calcium channel blockers need to be used with caution as
they can impair RV function.
LVAD use is ever increasing
in cardiology due to the increasing burden of heart failure patients.
Its use has changed
from being a bridge to transplantation to now being a destination therapy.
As a greater number of patients with heart failure have renal
dysfunction, LVAD use has implications for the nephrologist as well.
Post by Sriram Sriperumbuduri, Nephrology Fellow Ottawa