
Snake bite is a common and frequently devastating environmental and occupational disease, especially in rural areas of developing countries in tropical regions. Clinical manifestations depends on the dose of venom injected, bite to needle time, potency and adequacy of anti-venom. Envenomation may cause a very wide variety of complex effects, ranging from insignificant lesions at the site of the bite, to extensive local necrosis, and life threatening systemic effects of disseminated intravascular coagulation, acute kidney injury, acute respiratory distress syndrome, septicemia and sudden cardiac death from arrhythmia. Isoenzyme of the phospholipase PLA2 in snake venom is responsible for systemic manifestations of local capillary damage, tissue necrosis, and anticoagulant action. Complex clinical syndrome is characterized by hypotension, kidney injury, bleeding, and pituitary failure.
I saw a challenging case of Russell’s viper bite during my nephrology ward rotation. A fisherman was transferred with oliguric acute kidney injury (AKI) and history of Russell’s viper bite. He was in a critical conditions and was managed by supportive measures and hemodialysis. His hospital course was complicated by pituitary hemorrhage, following which he was put on hormone replacement therapy.
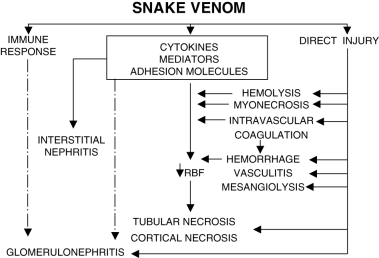
So, what are the renal manifestations in snake bite? Kidney is a highly vascularized organ and susceptible to venom toxicity. Clinical manifestations occur within few hours to 72 hours of viper bite. Renal features include loin pain, hematuria, hemoglobinuria, myoglobinuria, oliguria, and AKI. AKI is developed in up to 60% of Russell’s viper bite patients. Oliguria usually lasts for 4-15 days, and prolonged oliguria is common in elderly. Other manifestation may include acute interstitial nephritis, extra capillary proliferative glomerulonephritis and cortical necrosis. Mortality rates from snakebite-related AKI is estimated to be up to 35%. Recovery is usually complete except in cases with cortical necrosis or severe tubular necrosis with marked interstitial changes. The figure below elucidates the clinical presentation and pathophysiology of snake bite.
Management of snakebite includes first aid, local wound care, anti-venom and supportive measures. Immobilization of the whole patient, especially the bitten limb is needed, and transportation should be arranged to the nearing medical center. Tight tourniquets must be avoided so that limb loss is minimized. Anti-venom is the only specific treatment.
Supportive measures include
- correction of coagulopathy
- antibiotics for secondary infection
- fluid management
- dialysis support to AKI
- replacement of cortisol and thyroxine in hypopituitarism
Raising community awareness about prevention of snakebites is the most effective strategy for reducing snakebite morbidity and mortality. Concerted strategies with improvements in basic public health, region-specific guidelines and protocols, efficient preventive measures, increased access to effective medical care, adequate supply of anti-venom and timely referral of patients with established AKI to centers with dialysis facilities are essential to mitigate the preventable deaths from snakebite. WHO emphasizes on snakebite envenoming by comprehensive snakebite control strategy and international focus on neglected tropical disease snakebite to substantially improve the outcomes of the patients and communities.
NSMC Intern, Class of 2018


1 comment