RFN is proud to introduce a new series: “Kidney Biopsy of the Month.” We begin with normal histology of the kidney and specifically the glomerulus or renal corpuscle. After all, one needs to know what is normal before learning to recognize abnormalities. Distinguishing between normal and abnormal is not always easy.
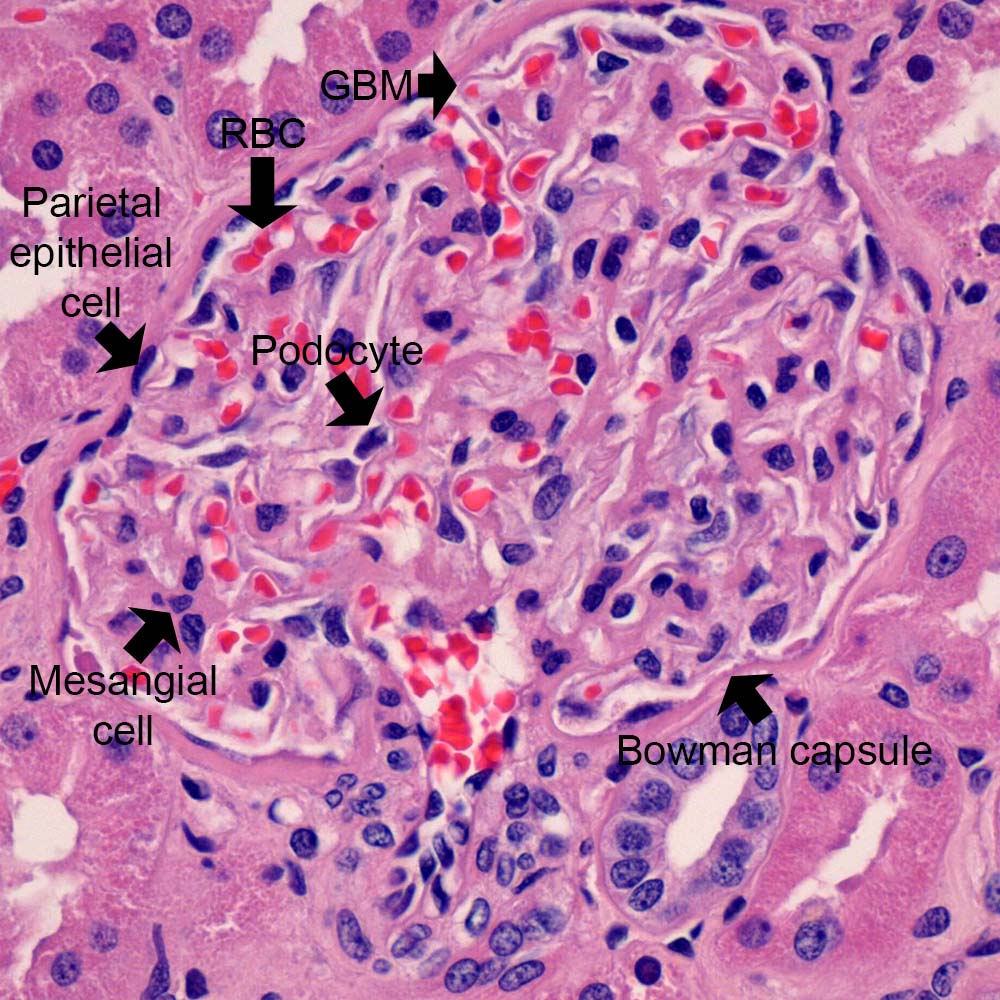
In general, we rely heavily on the Periodic acid-Schiff (PAS, Figure 1) and Jones methenamine silver (Figure 2) stains for visualization of glomeruli, as these histochemical stains highlight the glomerular and tubular basement membranes to define the different anatomic compartments of the kidney and glomeruli. Hematoxylin & eosin (H&E, Figure 3) nicely stains red blood cells, so thrombi may be easier to identify. The Jones stain is usually counterstained with H&E to provide some of that information in those tissue sections.
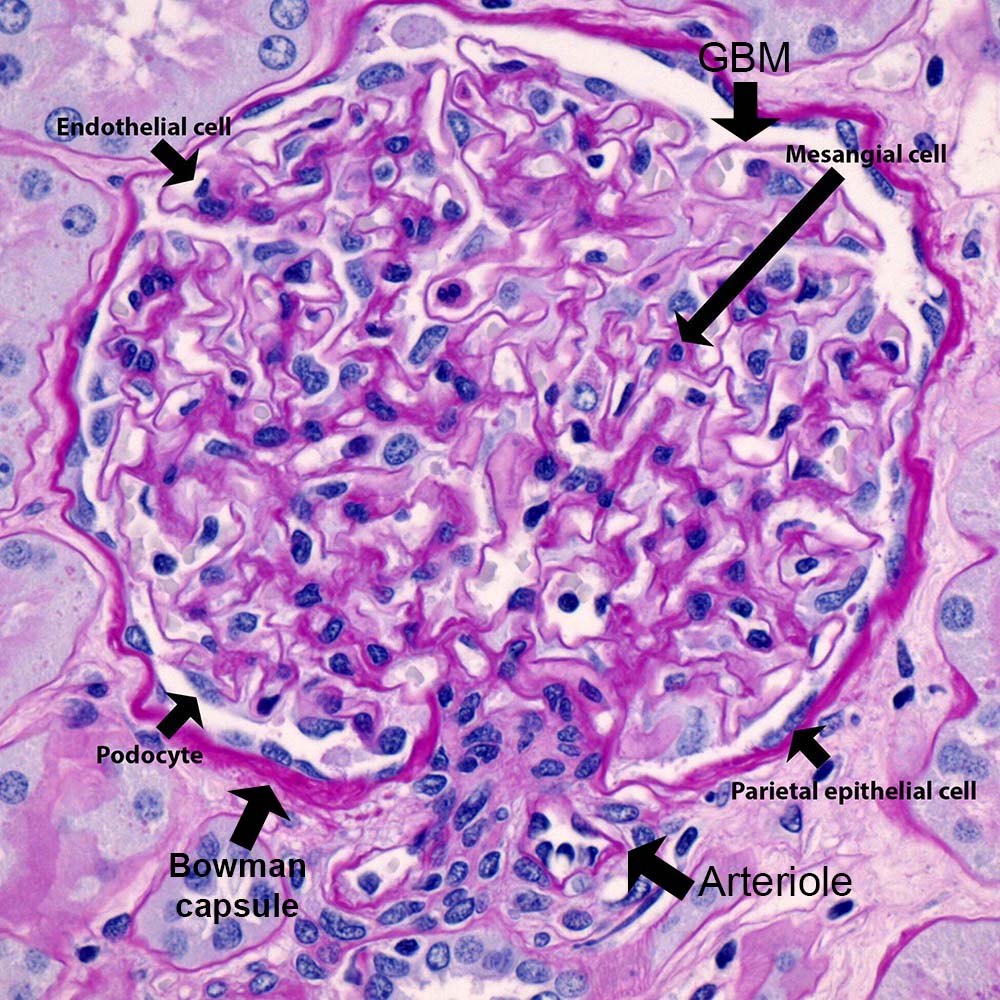
The average human glomerulus is up to 200 microns in diameter. Glomerular size is harder to assess without morphometry. One quick method that works for most microscopes – the glomerulus should not be more than half of the field of view when viewing with the 40X objective lens. The glomerular tuft consists of three cells types (mesangial, endothelial, and visceral epithelial cells – also known as podocytes).
Mesangial Cells
Mesangial cells are modified smooth muscle cells with phagocytic capability that can influence intracapillary blood pressure. Mesangial hypercellularity is defined as 3 or more nuclei per mesangial area when viewing a 2 micron thick tissue section. 4 or more nuclei per mesangial area is the criterion when viewing a 3 micron thick tissue section. The degree of cellularity should be assessed in the periphery away from the vascular pole where the region adjacent to the hilar arteriole can appear hypercellular. Mesangial matrix should surround the mesangial cell nucleus.
How much mesangial matrix is too much? This is difficult to define, but mild accumulation of mesangial matrix may indicate the presence of diffuse mesangial sclerosis (this may be an early manifestation of diabetic nephropathy or some other pathology). However, this finding should be presence in the majority of glomeruli in order for it to be of clinical significance. Caution: Ischemic glomeruli with fraying of Bowman capsule are often shrunken and can appear to have mesangial hypercellularity or mesangial sclerosis, but ischemic glomeruli should be ruled out when making this assessment.

Endothelial Cells
Endothelial cell nuclei protrude into the glomerular capillary lumen and these should not be included in the assessment for mesangial cellularity. The endothelial cells are fenestrated with fenestrae that measure 70-100 nm in diameter.
Visceral Epithelial Cells (Podocytes)
Podocytes are a terminally differentiated cell with complex processes that intertwine with adjacent podocytes along the glomerular basement membranes (GBM).
Parietal Epithelial Cells
The 4th cell type (parietal epithelial cell) lines Bowman capsules, but the lesser known parietal podocyte can also be found lining Bowman capsules and are more common near the vascular pole.
Glomerular Basement Membrane (GBM)
The GBM width typically averages between 300-350 nm and is contiguous with Bowman capsule. If the average GBM thickness is below 264 nm, then this satisfies the WHO definition for thin basement membrane nephropathy. The GBM anchors into the mesangial region (Figure 4, arrowhead). Detachment of this anchor results in 2 separate glomerular capillaries becoming one larger capillary, which occurs with mesangiolysis. The glomerular filtration barrier consists of the podocyte, glomerular basement membrane, and endothelial cell.

Post by: Anthony Chang, MD
Professor of Pathology, University of Chicago

Excellent and useful details about kidney staining. Much appreciated. thanks
thank you so much you saved my life i love your article
Thank for your article, it help me on my report!
Thanks a lot sir for explaining in such a nice and simplified way
Hi, May I use the first figure posted or is it copyrighted?
Thanks
Marti
Dr. Chang updated his post to include more markings. Thank you for the suggestion.
Thank you! Greetings from Colombia
We want to know more about nephropathology. please mark the important marking in all the slide. Thanks for posting