Anti-neutrophil cytoplasm antibody (ANCA) was first described in 1982 in a case of segmental necrotizing glomerulonephritis (Fig. 1). The first international ANCA workshop in 1989 delineated a standard immunofluorescence technique to test for ANCA in kidney biopsy specimen. During the second international ANCA workshop, the term “peri-nuclear ANCA” (p-ANCA) was accepted and soon after, ANCA serum antibodies assay were used as a diagnostic tool in ANCA glomerulonephritis.
ANCA-associated vasculitis (AAV) is now defined as a pauci-immune necrotizing vasculitis of predominantly small blood vessels that is associated with myeloperoxidase (MPO-ANCA), proteinase 3 (PR3-ANCA) positivity.
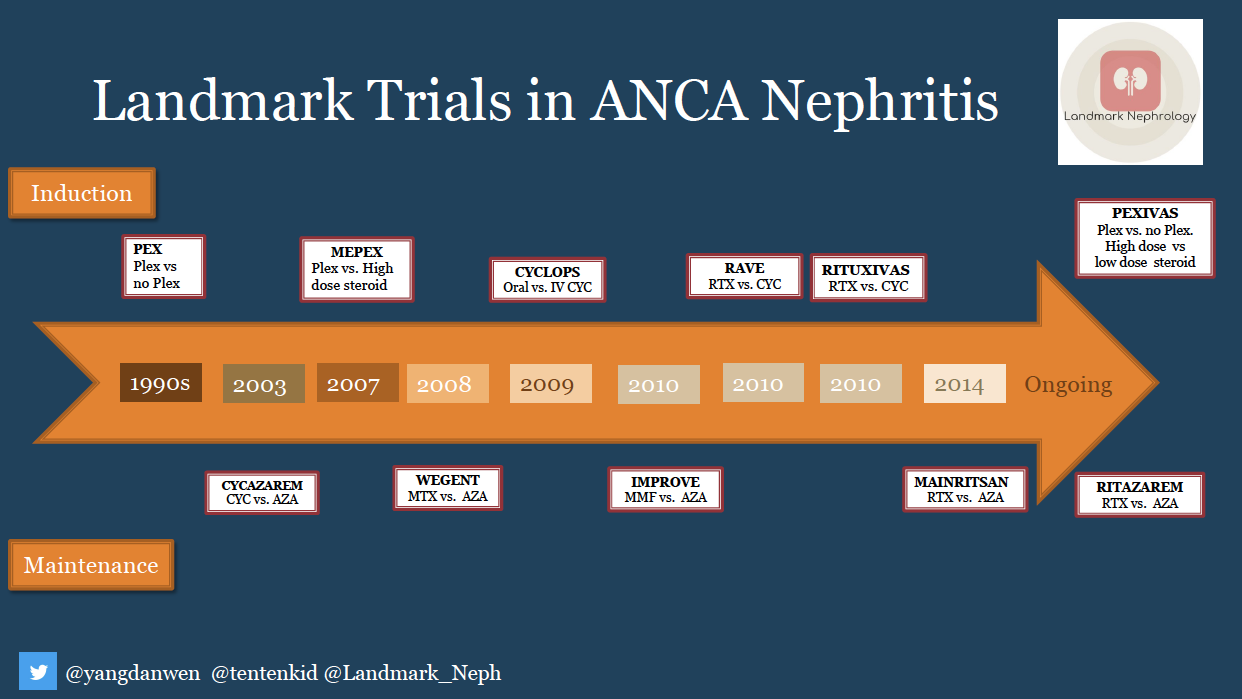
In this post, we’ll review the data that guide our treatment of AAV (Fig. 2).
Let’s start with cyclophosphamide and glucocorticoids:
Starting in the 1970s, cyclophosphamide (CYC) and glucocorticoids were found to be effective in ANCA vasculitis. Two decades later in 1992, a study of 158 patients with granulomatosis with polyangiitis (formerly known as Wegener’s granulomatosis) summarized that the outcome could be dramatically improved by daily treatment with cyclophosphamide and glucocorticoids, though disease-related and treatment-related morbidity were often profound, 13% of patients died, 86% of patients had irreversible features of their disease and 42% of patients had side effects of treatment.
In 2009, the CYCLOPS trial compared the effectiveness of oral versus intravenous (IV) CYC induction. Oral CYC was found to have lower rate of relapse, while IV CYC was more likely to induce remission and was associated with a significantly lower rate of leukopenia and infection. However, the study did not have enough power to detect a difference in relapse rates between the 2 groups.
What about rituximab (RTX)?
The RAVE trial compared RTX and CYC for induction, with each treatment given in addition to glucocorticoids. The trial showed that glucocorticoids plus RTX were not inferior to CYC for the treament of new onset AAV. Moreover, this regimen may be superior in relapsing AAV. Notably, in the RAVE trial, sicker patients including those with alveolar hemorrhage requiring mechanical ventilation or severe kidney failure with creatinine greater than 4.0 mg/dL were excluded. Subsequently, the RITUXIVAS trial showed similar data to the RAVE trial, with both treatment groups demonstrating a high rate of sustained remission but also with a high rate of severe adverse events. Notably in the RITUXIVAS trial, IV CYC was given with the first and third RTX infusions.
We anxiously awaited published data from the PEXIVAS trial: a 2×2 factorial randomized trial which compared plasmapheresis and standard vs low dose steroid for AAV with severe pulmonary and renal disease. All patients received either cyclophosphamide or rituximab. This trial may provide better data to inform treatment in the sickest patients.
Should we do plasmapheresis?
The role of plasmapheresis has been a recent area of debate in terms of hard outcome benefits. The first randomized study published in 1991 concluded that plasma exchange provided additional benefit to dialysis-dependent patients. However, the difference was less pronounced during a 12-month follow-up period. Similarly, in 2007, the MEPEX study showed reduction in risk of progression to ESRD in patients with serum creatinine >5.7 mg/dL, but again, subsequent analysis showed that the difference disappeared after 12 months. The PEXIVAS trial may also provide more data regarding a potential additive benefit of plasmapheresis.
Finally, maintenance therapy.
It has been established that induction therapy will need to be followed by maintenance treatment. The CYCAZAREM trial in 2003 showed CYC could be safely transitioned to azathioprine (AZA) for maintenance. The IMPROVE trial in 2010 suggested mycophenolate mofetil (MMF) was less effective than AZA for remission maintenance.
There may also be a role for rituximab for remission maintenance. The MAINRITSAN trial in 2014 showed that rituximab had better sustained remission at month 28th than AZA. Given the promising data, the RITAZEREM trial is ongoing to further investigate the role of rituximab as a maintenance therapy.
Looking back on the history of AAV treatment, it is exciting to see how the knowledge of AAV treatment has evolved and drastically changed AAV from a disease with 80% mortality to a chronic relapsing-remitting disease. Nevertheless, the optimal regimen of induction and maintenance treatment is yet to be determined.
Post by:
Natanong Thamcharoen, MD
Danwen Yang, MD
Landmark Nephrology is an online learning tool designed to collect landmark trials in nephrology and distribute content that makes learning nephrology fun and easy.
Please visit us to check out our topic-specific content including videos, visual abstracts, quizzes, and a new slide-share portal to facilitate the exchange of educational material within the nephrology community.
We love collaboration so contact us as landmarknephrology@gmail.com or find us on Twitter to get involved!


Wonderful. But little bit, provide more statistics details of each trial in short.
Thank you for making Nephrology easy & interesting