We learn the concept of ‘Fistula First’ since day 1 of fellowship. However primary failure rates have been rather high, with variable numbers reported in different literature. In addition, other complications related to AV fistula and AV graft cause significant patient distress and healthcare burden. Therefore, an awareness of those clinical presentations is of paramount important. In this article, we will go through different case scenarios that highlight the common complications associated with vascular dialysis access
Case 1
You arrive for your weekly dialysis rounds on a Monday morning and meet this pleasant 66 year old Woman who was recently established on at your dialysis unit. She is currently dialyzing through a RIJ tunneled dialysis catheter following an AKI on CKD IV about 7 months ago. Since she progressed to ESKD she had a brachiocephalic AVF created but it has failed to mature. The dialysis nurses are unable to cannulate her fistula.

1. What is the next step?
Having read our previous article about vascular access examination, you examine the access and diagnose an outflow issue. You refer the patient for a fistulogram.
2.What can be seen in this fluoroscopic image?
The cephalic vein segment in the upper arm is small and sclerosed.
3.What could have caused non-maturation?
You dig through the patient’s chart and realize that during her prolonged admission she had an ipsilateral PICC (peripherally introduced central catheter) placed. This case highlights the importance of preserving venous vasculature in advanced CKD patients. Other common causes of non maturation would include arterial insufficiency, central vein stenosis, presence of pacemaker or other lead wires causing venous obstruction and presence of accessory veins.
Diagnosis: Non Maturing AV
Case 2
You walk to the next patient and her dialysis machine is indicating a yellow light instead of green. You notice that the venous pressure is 300 mmHg with a blood flow of 400 ml/min. The spKT/V is 1.2. The patient is unhappy and tells you she is bleeding for 45 minutes at her radiocephalic AV fistula after dialysis. She has had the AVF for 4 years.
1.What should be the next step?
Again, the crucial vascular access examination should be done and you identify an outflow stenosis (failure of AVF to collapse on arm elevation test, augmentation test is normal and a high pitch bruit at the outflow tract is present).
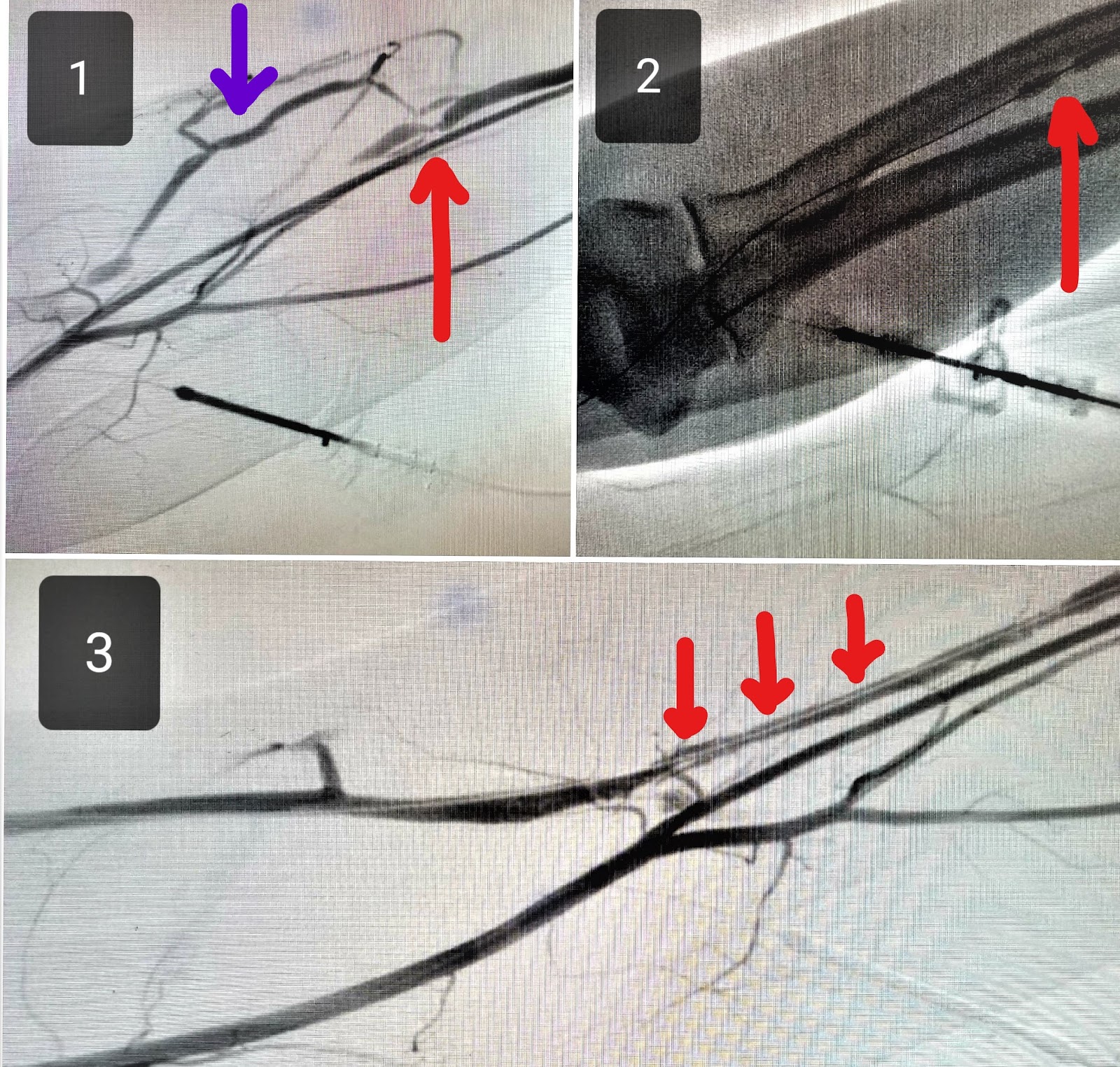
2.What can you observe in the fluoroscopic images?
Panel 1: Complete occlusion of outflow tract (red arrow) with a branching collateral vein (blue arrow)
Panel 2.Balloon Angioplasty with waist observed as balloon is being inflated.
Panel 3: Successful angioplasty with restoration of blood flow in outflow tract and elimination of collateral vein.
Diagnosis: Venous Outflow Stenosi
Case 3
You are the fellow on call on a Friday evening when you receive a page from the Emergency Room at 5.30 pm regarding an ESRD patient who presents to the hospital with shortness of breath, hypoxic respiratory failure needing NIPPV and hyperkalemia of 7.0 with peak T waves on EKG. During your assessment his wife tells you that he missed the last 2 dialysis treatments because of pain and swelling on his right arm. He is also having facial swelling with prominent dilated veins.

1.What can you observe?
A right upper arm AV fistula which appears dilated and tortuous with aneurysmal dilatation. He has prominent collateral veins, erythematous and tender right arm
2.What is the next step?
The patient should be scheduled for a fistulogram as soon as possible. He likely has central vein stenosis with possible SVC syndrome leading to the findings in the picture. It would be unsafe to use the fistula for dialysis as it may bleed uncontrollably following access. Also he will likely have significant recirculation leading to poor clearance. This patient may need a temporary dialysis catheter for emergent dialysis. In hindsight you realize that he had a pacemaker placed on the ipsilateral side but it was removed 1 year ago due to pocket infection. The wires were left in place.
Diagnosis: Central vein stenosis causing ‘Red hand Syndrome’ and ‘SVC syndrome
Case 4
A 68 year old male presents to the hospital with pain on his right arm. He has a right forearm radiocephalic AV fistula which was created 2 months ago and matured appropriately. The pain is aggravated during dialysis and is associated with tingling and numbness at the tips of his fingers. He has a history of peripheral vascular disease.

1.What do you observe on physical examination?
The right hand is pale and cyanotic. On palpation it feels cooler than his left hand. (Panel A).When you compare your hand to his, there is a clear difference in coloration. (Panel B)
2.What diagnostic test would you perform?
Allen’s test is positive and shows diminished blood supply from the radial artery. An upper extremity arterial doppler should be ordered to confirm the findings.
3.How do you treat this condition?
Vascular surgery should be consulted if your diagnostic tests are positive. This condition can result in limb loss if severe. In mild cases, observation may be sufficient, but in more severe cases, balloon angioplasty of the arterial supply may be needed. In the worst case scenario of acute ischemia, ligation of the AVF is required.
Diagnosis: Steal syndrome related to AV fistula. The 3 main causes are arterial occlusive disease, excess blood flow through the AVF, lack of adaptation or collateral flow reserve (atherosclerosis) to increased flow demand from the AV conduit
Case 5

You are attending weekly grand rounds when you get paged by the newly recruited dialysis nurse saying: ‘I am unable to cannulate the patient’s fistula. The patient is refusing dialysis, wants to give it rest. Please advise’. You go and assess the patient after the conference and you see this:
1.What is the diagnosis?
Infiltration around AVF with hematoma formation
2.What are the causes of infiltration?
Improper cannulation technique can lead to extravasation of blood around the access. Tight stenosis at the outflow tract can lead to the same. In those cases a fistulogram is required.
3.How do you manage this?
Rest and Ice packing is usually helpful in mild cases and cannulation may be attempted at the next dialysis session. In severe cases 4-6 weeks of rest is needed and an alternate dialysis access has to be established. If the AVF becomes dysfunctional due to hematoma, vascular Surgery should be consulted for evacuation and fistulogram.
Diagnosis: Infiltration.
Next week we will return with part 2 of this series, to discuss more cases related to complications associated with AV fistulas and grafts. Tune into RFN next Monday (April 1st).
Bhavnish Bucktowarsing, MD
ASDIN fellow
Acknowledgments: This post is part of a collaboration between the Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. Special thanks to Tushar Vachharajani, Aisha Shaikh, Edgar Lerma, and the Education Committee of ASDIN for their comments and suggestions for this post. For more information about the ASDIN mission or membership, click here. We would also like to thank Anil Agarwal, Robin Shah, Nabil Haddad, Khaled Boobes for assisting with this post.
Please note: these cases are vignettes created for educational purposes and patient consent has been obtained by author for clinical images.


Thanks for a wonderful post.
My doubt pertains to case 5- how to differentiate between mild and severe cases of infiltration around AV fistula( terms mentioned in management aspect of infiltration case).