The general notion is that edematous states like acute decompensated heart failure (ADHF) respond to the combination of sodium restriction and diuretic therapy. In fact, non-adherence to sodium restriction is believed to be a primary cause of failure to diuretic response. This failure to achieve euvolemia despite a therapeutic dose of diuretic is called diuretic resistance. Paradoxically, there is evidence that the combination of diuretics and intravenous sodium supplementation, in the form of hypertonic saline solution (HSS), can overcome diuretic resistance in patients with ADHF.
This subject was previously discussed in #NephMadness 2015: Sodium Restriction for Congestive Heart Failure (CHF) vs Hypertonic Saline in Acute CHF, take a look!
Part 1. More Salt For Volume Overload?
When I was an internal medicine fellow in 2011, there was a senior cardiologist who prescribed hypertonic saline followed by high dose furosemide in a patient with ADHF. In our evidence-based academic hospital, this counterintuitive therapy was seen as adding fuel to the fire. I decided to dive into the medical literature to see if there was evidence to back-up the practice and I discovered the work of Salvatore Paterna.
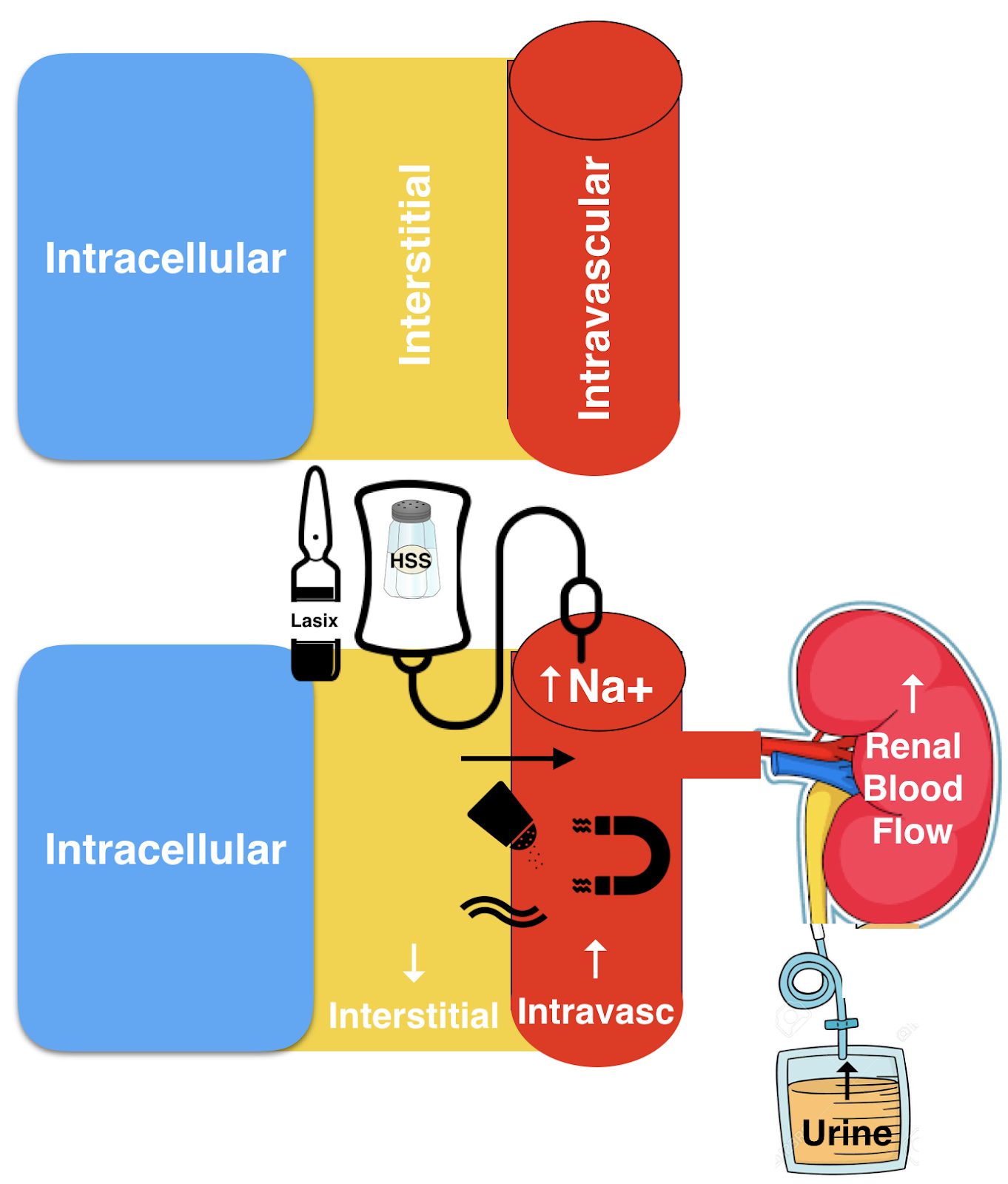
The earliest work was an exploratory study from 1999 about treating heart failure with 150 ml of hypertonic saline (NaCl 1.4–4.6%) according to serum sodium values plus 250 mg IV furosemide twice a day. They showed that this strange concoction was both safe and tolerated. The rationale behind this combination was to overcome diuretic resistance by using the hypertonic saline to draw water from the interstitial compartment, thus improving effective arterial blood volume and renal blood flow and counter the deleterious effects of furosemide by suppressing rather than activating the RAAS.
The proposed mechanisms included volume expansion by hypertonic saline as a resuscitation fluid leading to the mobilization of fluid to the intravascular compartment followed by increased urine output (Figure 1). Additional effects include enhanced myocardial contractility, peripheral vasodilatation, improved neuro-hormonal profile, and increased renal blood flow. It is also hypothesized that the sodium chloride increase sensed by the macula densa may also play a role in increased diuresis.
These initial studies were followed by a series of small studies in 2000, 2003, 2005, and culminated with 2011’s SMAC-HF study. SMAC-HF was a single center randomized blinded-study (N=1927) comparing HSS with furosemide and a moderate sodium diet (120 mmol or 2760 mg) versus furosemide alone and a low sodium diet (80 mmol equivalent or 1840 mg). The HSS group had a shorter hospitalization (3.5 vs 5.5 days), improved NYHA class, lower readmission rate (~19% vs ~34%), and reduced CV mortality (~13% vs ~24%).
These surprising results from this unconventional treatment caught my attention. Maybe sodium was like beta-blockers in heart failure, a treatment that was contraindicated for years before someone give it a chance and now has become an evidence-based treatment widely recommended.
Dietary sodium was also an intervention in this study. It is important to recap this controversy. The average sodium intake in the US population is over 4 g per day. In 2014 the Institute of Medicine convened an expert committee to evaluate the evidence about the health effects of low sodium intake (<2.3 g per day or <1.5 g per day). The committee found limited evidence that low salt intake is associated with an increased or reduced risk of cardiovascular disease in the general population but may be associated with adverse health effects in some subgroups, including some patients with heart failure or other forms of cardiovascular disease, diabetes, or chronic kidney disease.
In summary, we need stronger evidence to better understand the effects of HSS therapy and low sodium diets.
Part 2. A Case Experience
Fast forward years later, during my nephrology fellowship, when the evidence in ADHF suggested a stepped pharmacologic approach. Our patient was an individual with ADHF with new onset acute kidney injury (AKI) resistant to high-dose diuretic combinations. It seemed like ultrafiltration was the next step. I recalled HSS, the ace up my sleeve. We discussed it with the patient and he agreed.
Our patient characteristics fit the inclusion criteria from previous studies:
- New York Heart Assocation (NYHA) Heart Failure Class III-IV
- Low ejection fraction (EF)
- Previous medications (angiotensin converting enzyme inhibitors, Nitrates, Digoxin)
- Use of furosemide/spironolactone with diuresis of less than 800 ml/day
- Cr <2.5mg/dl, BUN <60 mg/dl.
We prescribed 150 ml of 1.4% NaCl with 250 mg of furosemide, twice daily along with potassium supplementation (20-40 mEq/L/d). We also enforced a moderate sodium restriction and limited fluid intake to a liter a day. The daily diuresis increased to 2.5-3.5 L over the next 3 days and my patient soon reached a compensated state. This patient required frequent monitoring. The infusion was stopped, replaced with high dose oral diuretics and he was discharged without subsequent rehospitalization.
We should be very careful on worsening volume overload (risk of pulmonary edema), hyponatremia overcorrection and causing hypokalemia or metabolic alkalosis.
Part 3. Back to the evidence.
Does HSS with furosemide improve outcomes for patients with ADHF?
In a 2014 systematic review and meta-analysis of 10 single and double-blinded RCTs comparing furosemide and HSS versus furosemide alone in patients with ADHF demonstrated decreased all-cause mortality in patients treated with HSS. The analysis also revealed decreased heart failure hospital readmission and preservation of renal function. The majority of the trials were from the same center, limiting conclusions from the meta-analysis.
Do we have studies from other centers?
A Canadian study of 47 patients admitted with ADHF showed that the administration of HSS with furosemide led to greater weight loss compared to the intravenous furosemide strategy alone. This population included people with heart failure with preserved ejection and others with advanced kidney failure.
A randomized single-blinded study (N=43) in Turkey compared three diuretic regimens for ADHF:
- Furosemide 160 mg infusion over 16h per day
- Furosemide 80 mg bolus injections twice daily
- Furosemide 160 mg bolus plus 150ml of 1.95% HSS once daily
The HSS group compared with the continuous infusion and bolus groups had shorter hospital stay with no difference in weight loss.
Yoshitaka et al showed that the addition of hypertonic saline (500 ml of 1.7% NaCl) to low dose furosemide (40mg) enhanced diuresis compared with control (IV glucose) and low dose furosemide. They also found increased creatinine clearance.
Is there a renoprotective effect of HSS?
In a case-control study from Italy enrolled 15 patients and 38 controls showed that HSS was protective against the decline in kidney function induced by loop diuretics. However the same nephroprotection was not seen in in patients with baseline creatinine over >2.2 mg/dL.
This was confirmed in the only randomized, double-blind study (N=50) in ADHF and advanced kidney disease population (Cr >2mg/dl, BUN >60mg/dl) who compared HSS 2.4% saline with 250mg furosemide and 0.9% saline with 80mg furosemide. The HSS group led to a non-significant better diuresis but also BUN elevation from baseline.
In conclusion, these studies undoubtedly challenge our understanding and practice of sodium restriction and simultaneously tempt us to administer hypertonic saline in ADHF. Moving forward, we should be open to challenging existing and be open to learning about new approaches. However, at this moment there is insufficient data to routinely administer hypertonic saline in this population or liberalize oral sodium intake.
Post by: Aldo Rodirigo Jiminez Vega, MD
NSMC Intern, 2019


Thanks for the comprehensive review. I would like to point out that the rationale of this approach is not enabling drawing of water from interstitial to intravascular, rather movement of water from intracellular (IC) to extracellular (EC) and thus both interstitial and vascular space. HS works by raising osmolarity of EC space (interstitial and vascular compartments are separated by semi-permeable capillary membrane and HS distributes in 3/4 and 1/4 proportion respectively, in these compartment, being a small molecule 23 dalton), and then high EC osmolarity moves water from IC to EC by stimulating cellular aquaporin channels.
Has any of the study examined the total sodium balance after having administered 154 meq of extra sodium (300 ml of 513 meq/L) per day?
The data discussed in the above article is insufficient based on small number of patients. The similar results can be achieved by infusing albumin with diuresis.
Absolutely amazing review of the topic and great explanation of the proposed pathophysiology. Thank you so much for doing this! Extremely helpful!
This is really an excellent comprehensive overview of the subject, thanks