Several drugs, mainly antimicrobial or antiviral agents, can cause transient crystalluria, in isolation or in conjunction with other urinary abnormalities and a wide range of clinical implications. The factors favoring the formation of drug crystals are drug overdose, dehydration, hypoalbuminemia, high or low urine pH. An important risk factor for the development of acute kidney injury (AKI) is the presence of an underlying kidney impairment [1,2]. Table 1 summarizes the different types of drug crystals reviewed below.
Table 1. Examples of Drug Crystalluria
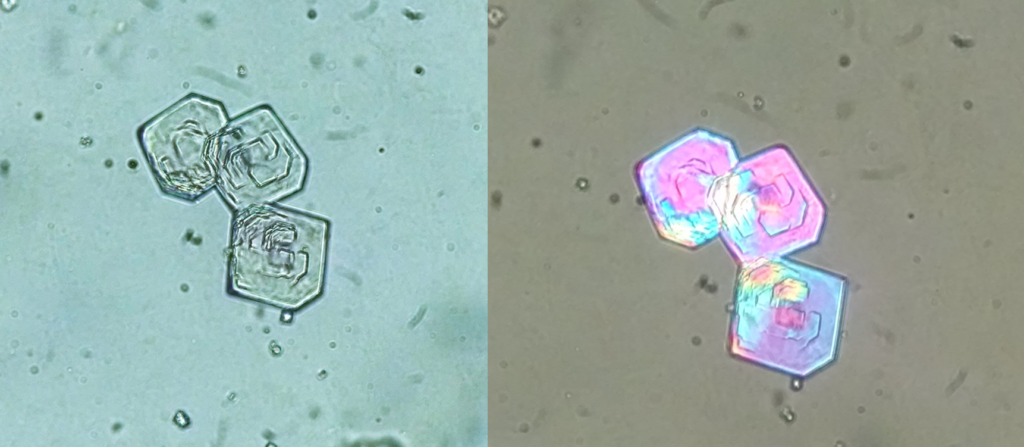
Some sulfonamides may induce crystalluria. One such drug is N-acetylsulfamethoxazole chlorhydrate, a metabolite of sulfamethoxazole which is widely used in combination with trimethoprim. Crystals, which precipitate at a pH around 5.0, may have the shape of lozenges, hexagons (Figure 1) or ovoid structures, which mimic uric acid dihydrate, cystine or whewellite, respectively [2,3]. Key information to be able to properly identify this kind of crystal is: (a) the knowledge of patient’s medications and (b) the observation of the crystals polarization properties under polarized light microscopy.
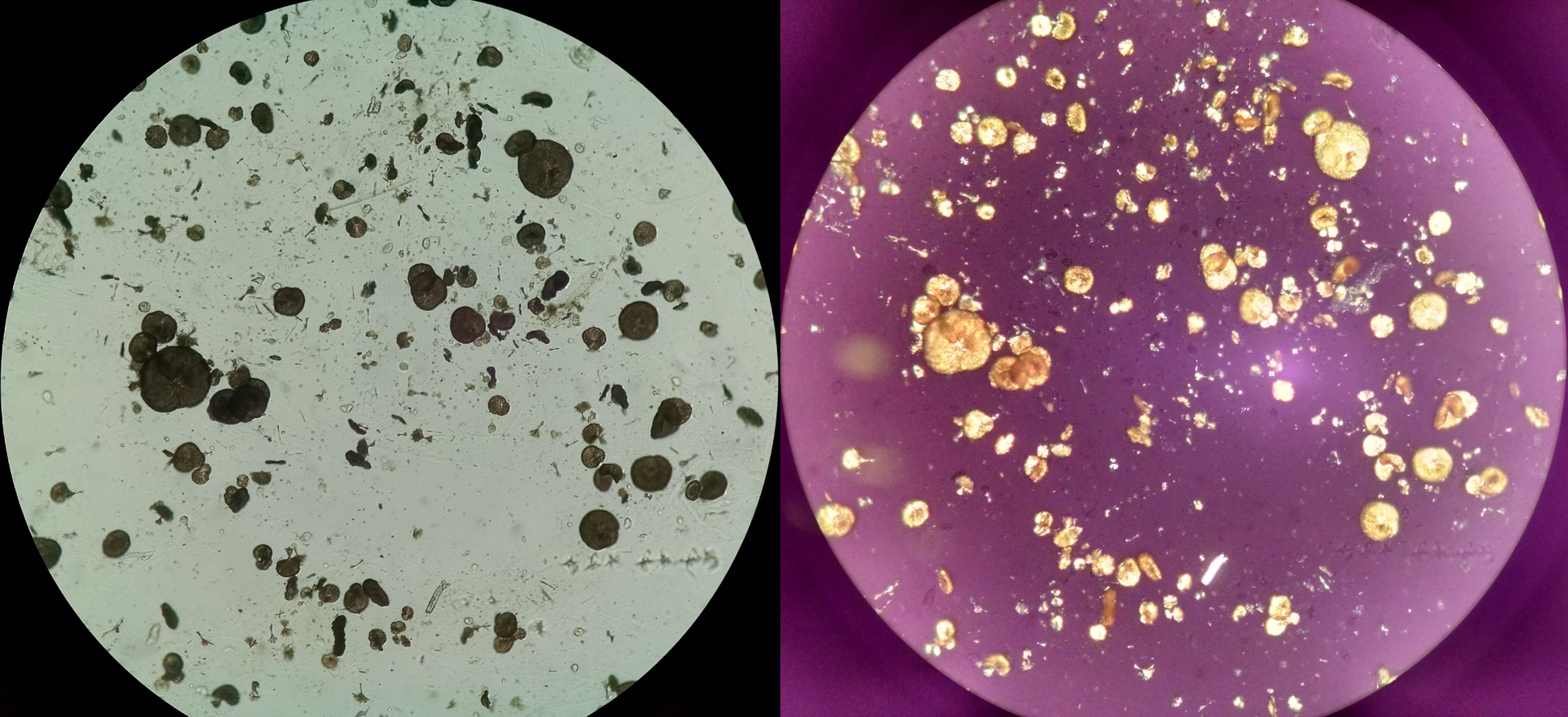
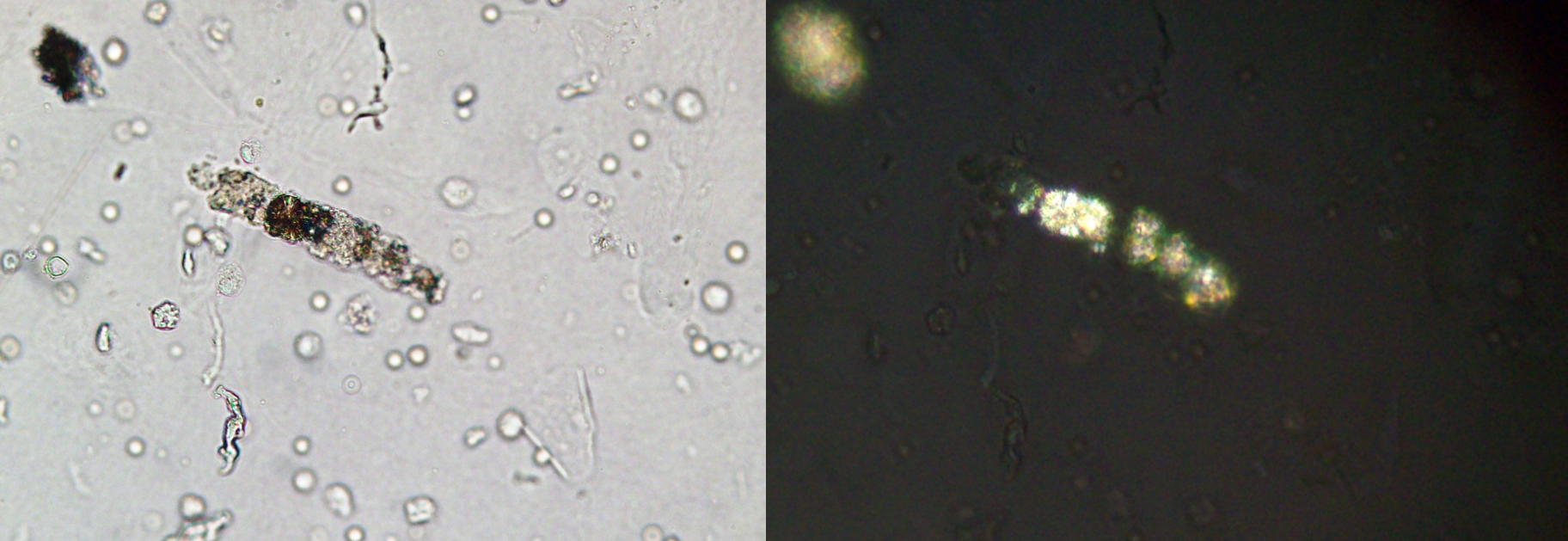
N-acetylsulfadiazine, a metabolite of sulfadiazine (Figure 2) used in the treatment of cerebral toxoplasmosis, also crystallizes in acidic urine [2]. It is important to mention that drug crystals can be observed within urinary casts (Figure 3), a clear sign of intratubular precipitation and a clue to the identification of drug-related-AKI [4].
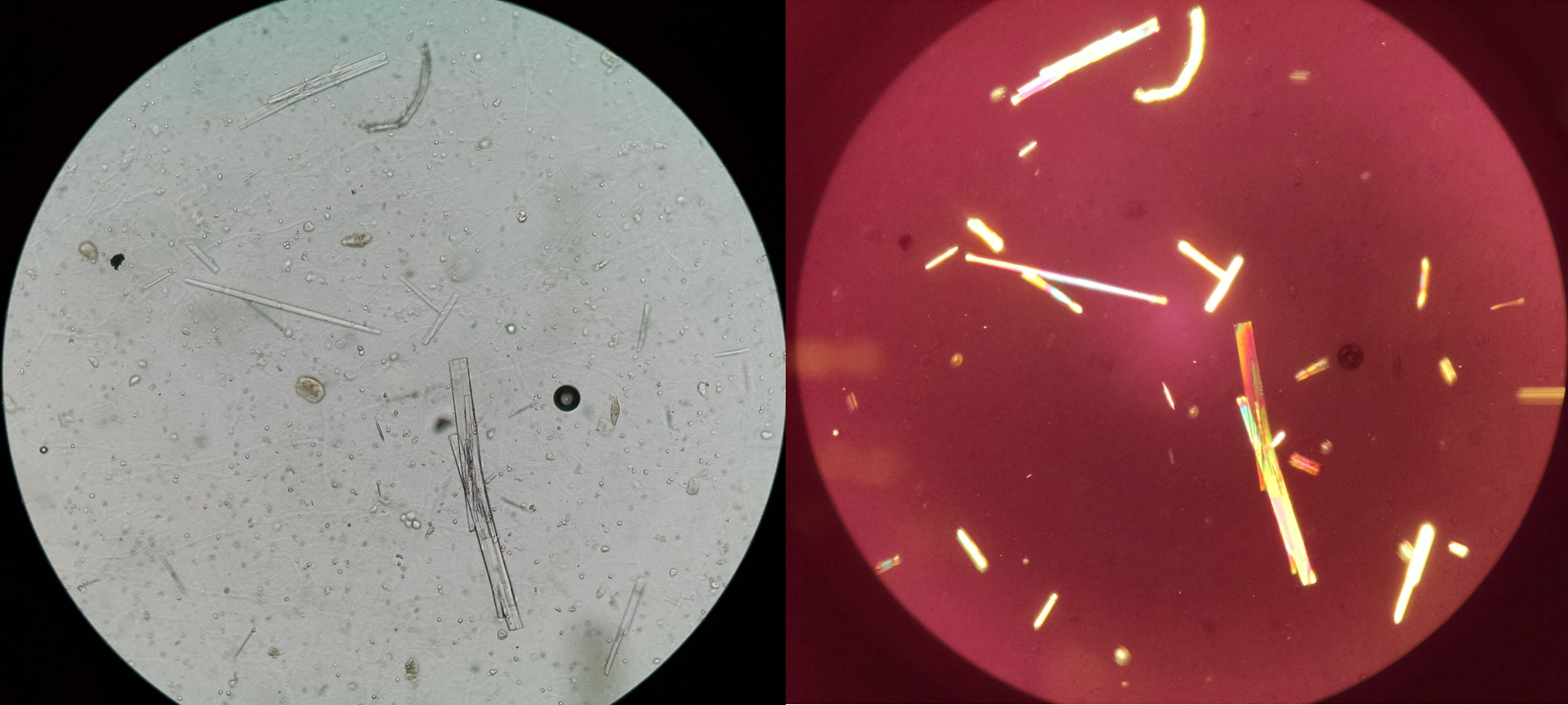
Other antibacterial agents such as aminopenicillins (particularly amoxicillin (Figure 4)), fluoroquinolones and, more rarely, ceftriaxone may induce crystalluria, which at times may be associated with AKI due to the intratubular precipitation of crystals [2,4].
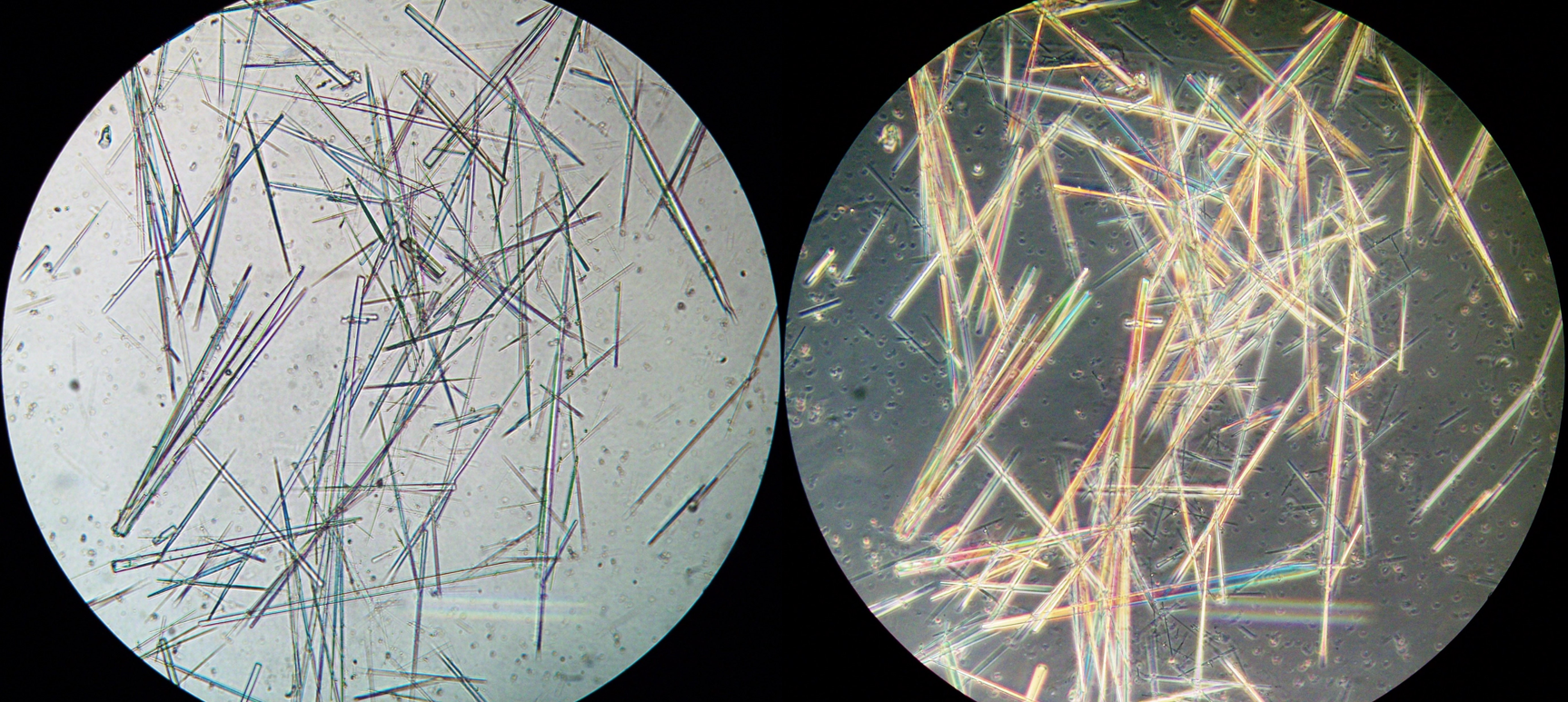
Antiviral agents currently are a common cause of crystalluria, especially atazanavir. Acyclovir (Figure 5), used in the treatment of herpes virus infections, also forms crystals with an aspect of long, thin needles that may form aggregates [2].
Other drugs which may cause crystalluria are indinavir, triamterene, primidone and felbamate, whose crystals have most unusual and pleomorphic morphologies, a fact which should alert the urine microscopist [2].
Other drugs such as naftidrofuryl oxalate, orlistat and vitamin C, when given intravenously at high doses, may also cause urinary crystals, which are made up of calcium oxalate indistinguishable from calcium oxalate crystals from other causes [2].
Urinary crystals due to drugs (in the major part of cases observed as thin needles) are an uncommon finding, usually are not linked to kidney injury (but they can be!). When they occur, they are commonly a source of doubt to analysts. Without information on medication administration and without use polarized light filters, the proper identification can be extremely challenging.
References:
- Fogazzi GB. The urinary sediment an integrated view. 3rd edition. Elsevier, 2010.
- Daudon, M., & Frochot, V. (2015). Crystalluria, Clinical Chemistry and Laboratory Medicine (CCLM), 53(s2), s1479-s1487.
- de Liso F, Garigali G, Ferraris Fusarini C, Daudon M, Fogazzi GB. How to identify sulfamethoxazole crystals in the urine. Clin Chim Acta. 2016;452:106‐108.
- Poloni JA and Perazella MA. Clinical Journal of the American Society of Nephrology cover image, January 2013. What’s the diagnosis.
Post by: José A. T. Poloni