Learning points
- Anatomical variation is high in parathyroid glands
- In medication resistant hyperparathyroidism associated with kidney disease, surgical exploration is key. Imaging is a useful adjunct to localise ectopic or supernumerary parathyroid glands
- Hyperparathyroidism causes bone resorption, calcific deposition and osteosclerosis
Case
A 38yo male with ESKD due to hypoplastic kidney disease. There was no history of previous parathyroid surgery. His results were significant for:
- PTH 103 pmol/L (936pg/mL)
- ALP 200 U/L
- Calcium 2.44 mmol/L (9.76mg/dL)
- Phosphate 2.98 mmol/L (9.23mg/dL)
A Tc99m MIBI SPECT/CT was performed:

Two parathyroid adenomas were reported: one posterior to the right inferior thyroid pole and the other posterior to the left superior thyroid pole. There were no ectopic glands. An ultrasound was also performed. It was able to also confirm both these masses, and potentially a third.
Ultimately, surgical exploration demonstrated all parathyroid glands to be hyperplastic weighing between 150 and 870mg.
This case highlights the primacy of surgical exploration. While imaging was able to eliminate the possibility of ectopic glands, intraoperative assessment confirmed hyperplastic rather than adenomatous parathyroids.
Parathyroid Anatomy
There are typically 4 parathyroid glands. Each gland is small: approximately 5x3x1mm and weighs about 50mg, and therefore infrequently identified on imaging. On the other hand a parathyroid adenoma is usually 10 times heavier than normal, weighing up to 20g. The hyperplastic glands of hyperparathyroidism associated with kidney disease are variable in size but tend to be smaller than adenomas. There is overlap in size between normal and hyperplastic glands.
The superior glands are deep in the mid-superior pole of the thyroid near the cricothyroid junction in 90% of cases. The inferior glands are inferior, posterior or lateral to the lower thyroid pole in 70% of cases (Figure 1).
However, the parathyroid glands are variable in location and number. They can be found as superiorly as the carotid bifurcation, as inferiorly as the pericardium, as posteriorly as retro-esophagus, and as anteriorly as the thyroid. Supernumerary glands exist in 12%, and fewer than 4 glands occur in 3% of people. Therefore there is approximately a 50% chance of an anatomical variation in any one patient.

Figure 1. Typical positions of the parathyroid glands. Note the position of the superior parathyroids posterior to, and inferior parathyroids anterior to the recurrent laryngeal nerve. Injury to the nerve causes hoarseness of voice.
Imaging Modalities
Sestamibi Scan- Technetium 99m (Tc99m) sestamibi is the modality of choice. It localises in the increased number of mitochondria in parathyroid cells. That is, it is increased in tissues with a high metabolic state.
Thyroid tissue is also metabolically active especially in some nodules. There are a number of solutions to differentiate the parathyroids from thyroid:
- Dual phase MIBI – Scans are done 15 minutes (early), then 2 hours (delayed images) after injection. Tracer washes out from normal thyroid tissue more rapidly than hyperplastic parathyroid. Hyperplastic parathyroid tissue characteristically demonstrates increased tracer uptake greater than the thyroid in the early images, and continued retention in the delayed images whereas the tracer in the thyroid tissues are washed out.
- Comparing images taken with Tc99m MIBI and Tc99m pertechnetate (TcO4) or iodine-123 (I123). Tc99m MIBI highlights thyroid and parathyroid glands, while TcO4 and I123 only highlights thyroid. Subtraction is then performed between the images to display the parathyroids.
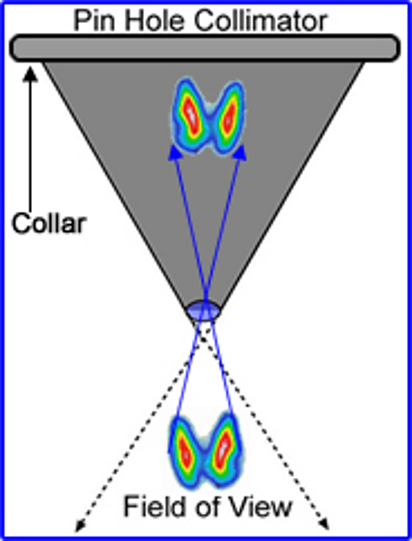
Further, a pinhole collimator can be used to enhance sensitivity. It acts as a magnifying glass over the thyroid and parathyroid area to increase sensitivity. It looks like:
Preparation
For most patients no preparation is required
- In patients on very high doses of Vitamin D and calcimimetics, these drugs may lower Tc99m MIBI uptake and therefore decrease sensitivity of the test
- If using I123 or TcO4, stop thyroid hormone replacement for 3-4 weeks as this interferes with thyroid uptake values
- Do not perform test after IV radiologic contrast
Special population – Pregnancy
Fetal radiation dose of parathyroid MIBI is typically <5mGy, which is well below the concerning threshold (ACOG). Another strategy is to halve the dose of radioactive tracer and compensate by doubling the gamma camera acquisition time. However, radioactive iodine should be avoided. This may cause fetal hypothyroidism. If breastfeeding, no interruption is required for those administered Tc99m MIBI, 12 hours and 3 weeks interruptions are required respectively for those administered TcO4 and I123 .
Sestamibi results in a planar images (Figure 3A):
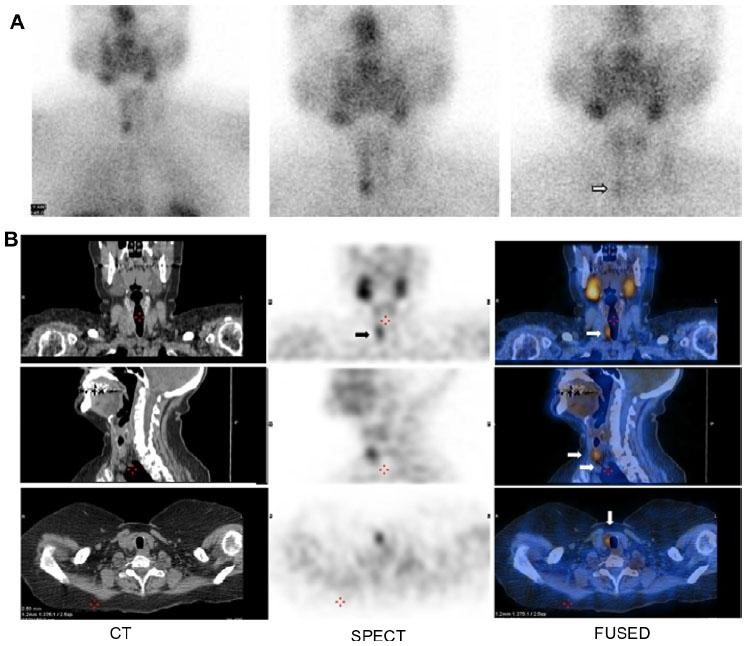
Figure 3A) A focus of increased uptake at the right lower pole seen on the early image and persisting on the delayed image (arrow) which showed further clearance of thyroid background activity. SPECT/CT study (B) was also obtained, showing the lesion with better contrast and anatomic localization (arrow)
The sensitivity of sestamibi in secondary hyperparathyroidism is mediocre, and ranges between 56 to 75%. Therefore there is practice variability in ordering preoperative imaging prior to parathyroidectomy. However it is especially useful after operative failure to identify lesions and to localise ectopic or supernumerary glands. Surgical exploration may mistake hyperplastic glands for nodular thyroid tissue. Supernumerary glands are the main cause of persistence (up to 10% of cases) resulting in early hyperparathyroid recurrence. Functional imaging may also guide the surgeon towards the most suitable gland for preservation. Size correlates poorly with PTH levels, that is, a small sized hyperplastic parathyroid can be more active than one with a larger mass.
SPECT/CT– This uses the same gamma camera as Sestamibi, with a simultaneous CT in order to localise the parathyroids onto a 3D image. This is especially useful to pinpoint the position of mediastinal and ectopic parathyroid glands (Figure 3B)
Ultrasound– Ultrasound does not commonly reveal normal or hyperplastic parathyroids (as in renal patients) due to their small size. Therefore it is most useful in uniglandular disease (eg parathyroid adenomas)
MRI– Use is limited. T1 and T2 characteristics of abnormal tissue are variable, and gadolinium enhancement has not been shown to be helpful. Further, abnormal parathyroid tissue can also have similar characteristics as lymph nodes.
X-ray– These can illustrate peripheral consequences of hyperparathyroidism including:
- Resorption
- Subperiosteal
- Subchondral
- Subligamentous
- Intracortical
- Terminal tuft erosion (acro-osteolysis)
- Salt and pepper sign
- Brown tumours (osteoclastomas) – Usually involve bones of the face, pelvis, ribs and femora
- Deposition
- Soft tissue
- Chondrocalcinosis
- Osteosclerosis
- Rugger jersey spine – Alternating bands of hyper and hypodensity of the spine.

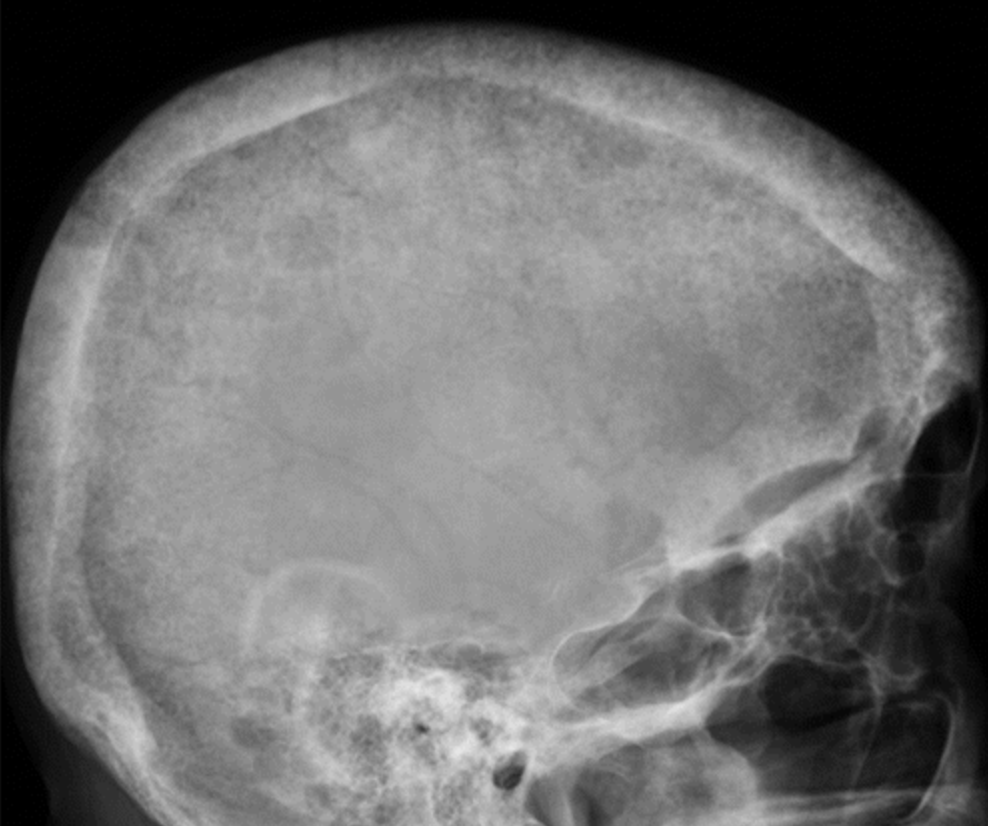
Figure 7. Rugger jersey spine – Alternating bands of sclerosis along the endplates (dashed arrows) and areas of lucency centrally (solid arrows)
Figure 8. Soft tissue deposits (arrows in the dorsal forearm)
Dr Jian Cheng, Nephrologist
Orange Base Hospital, NSW Australia
@Urinecredible1
Thanks to Drs Mirna Vucak-Dzumhur (CKD-MBD nephrologist) and Simon Gruenewald (radiologist) from Westmead Hospital, Sydney Australia; and Dr Matt Sparks for their input