Orhan Efe
Nephrology Fellow
Brigham Womens Hospital/Massachusetts General Hospital Program
Harvard Medical School
Background and Basics
The goal of transplant evaluation is to identify suitable candidates who would benefit from transplantation. To accomplish this goal, a multidisciplinary team is required. This team is typically comprised of a transplant nephrologist, surgeon, coordinator, pharmacist, social worker, and nurse coordinators. Transplant referral should be considered when eGFR<30 to allow timely evaluation and identify potential living donors. In the US, suitable patients can be waitlisted to the United Network for Organ Sharing (UNOS) when eGFR<20.
Currently, wait time for the listed candidates is 3-7 years, varying according to geographical location, blood type (higher in O and B) & sensitization status of the patients. For the patients who are listed late, pre-registration dialysis time counts for wait time retrospectively but pre-dialysis low GFR duration is not included. Hence, early referral is particularly important for pre-dialysis patients.
| Absolute Contraindications to Kidney Transplantation | Relative Contraindications |
| Active medication noncompliance | Active systemic diseases (e.g. SLE, ANCA) |
| Active malignancy | Uncontrolled tertiary hyperPTH (parathyroidectomy first) |
| Active infection | Primary oxalosis (refer to combined kidney-liver) |
| Active substance abuse | Systemic amyloidosis, especially with cardiac involvement |
| Uncontrolled psychiatric disorder | Early failure of prior transplant due to recurrent disease |
| Severe bilateral iliac or lower-extremity arterial disease | Severe ischemic cardiomyopathy with EF<30% |
Assessment
A detailed history continues to remain a crucial component of the recipient evaluation. Assessment of underlying etiology of kidney failure is important to assess risk of recurrence in the allograft. A detailed family history can aid in ascertaining recipient’s kidney disease etiology and potential living donors, while a surgical history determines anatomic feasibility of transplantation. It is imperative to assess a patient’s social environment, support system, and factors that may affect medication compliance. In addition, it is noteworthy that age alone is not a contraindication but elderly patients should be evaluated for frailty which increases mortality after transplantation.
Sensitization assessment requires estimation of exposure to non-self HLA antigens via transfusion, pregnancy and prior transplant may result in the development of anti-HLA antibodies. Lastly, assessing the comorbidities (further below) such as oncologic and psychiatric history, along with previous viral exposures and immunization are also vital.
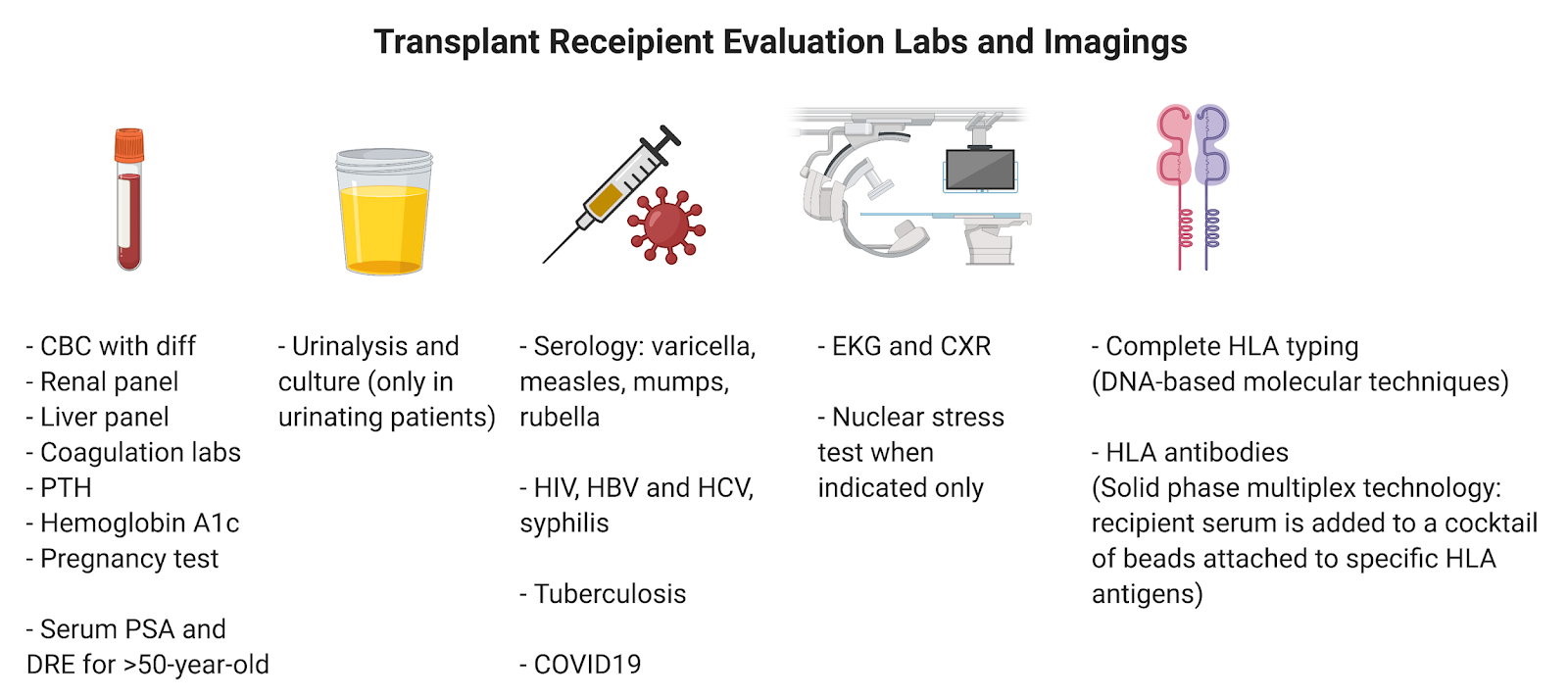
With regard to testing, human leukocyte antigen (HLA) alleles should be identified for each candidate. HLA-A, HLA-B, HLA-DR alleles (2 alleles for each) are used for antigen mismatch scoring (between 0-6) which is a main determinant of prioritization in organ offering. In addition, preformed antibodies against specific HLAs should be tested at initial evaluation and then periodically as it is a key risk factor for antibody-mediated rejection. Commonly performed other tests are summarized in figure 1.
Evaluation of Comorbid Conditions
Cardiovascular disease and malignancies are two commonly encountered comorbidities which are very important to evaluate before listing any recipient.
Cardiovascular Disease (CVD): CVD is the most common cause of death (30%) in transplant recipients which is due to both peri-operative and long-term risk. Patients with no CVD disease or risk factors do not require any cardiac investigation. On the other hand, patients with known CVD or who have diabetes or poor functional status are suggested to have evaluation with non-invasive cardiac stress test as per KDIGO. The AHA recommends non-invasive stress test in patients with 3 or more risk factors including diabetes mellitus, prior cardiovascular disease, more than 1 year on dialysis, left ventricular hypertrophy, age greater than 60 years, smoking, hypertension, and dyslipidemia. Patients with positive findings should undergo coronary angiography. In terms of cardiac function, patients with uncorrectable, symptomatic NYHA III/IV heart failure (e.g. EF<30%) should be excluded from kidney transplant (KT) and considered for combined heart-kidney transplantation per KDIGO. Lastly, patients with irreversible moderate to severe pulmonary hypertension should be excluded from transplantation. Milder cases can be assessed by a cardiologist for the risks of progression after KT and life expectancy.
Malignancy: All patients should undergo age-appropriate cancer screening. Patients with preexisting malignancies have higher cancer-associated and all-cause mortality. Suggested wait time for these patients differs between cancer types which is determined by the risk of recurrence and mortality. For very low or low risk cancers such as basal cell carcinoma and in situ breast cancer, usually no waiting time is advised. For prostate cancer, patients with even high stage disease without metastasis may be transplanted with no waiting time if their 15-year mortality is <10%. For high risk malignancies such as stage III breast cancer and stage III colon cancer, suggested waiting time is up to 3-5 years. Overall, especially for higher stage malignancies, a team decision involving an oncologist should be sought.
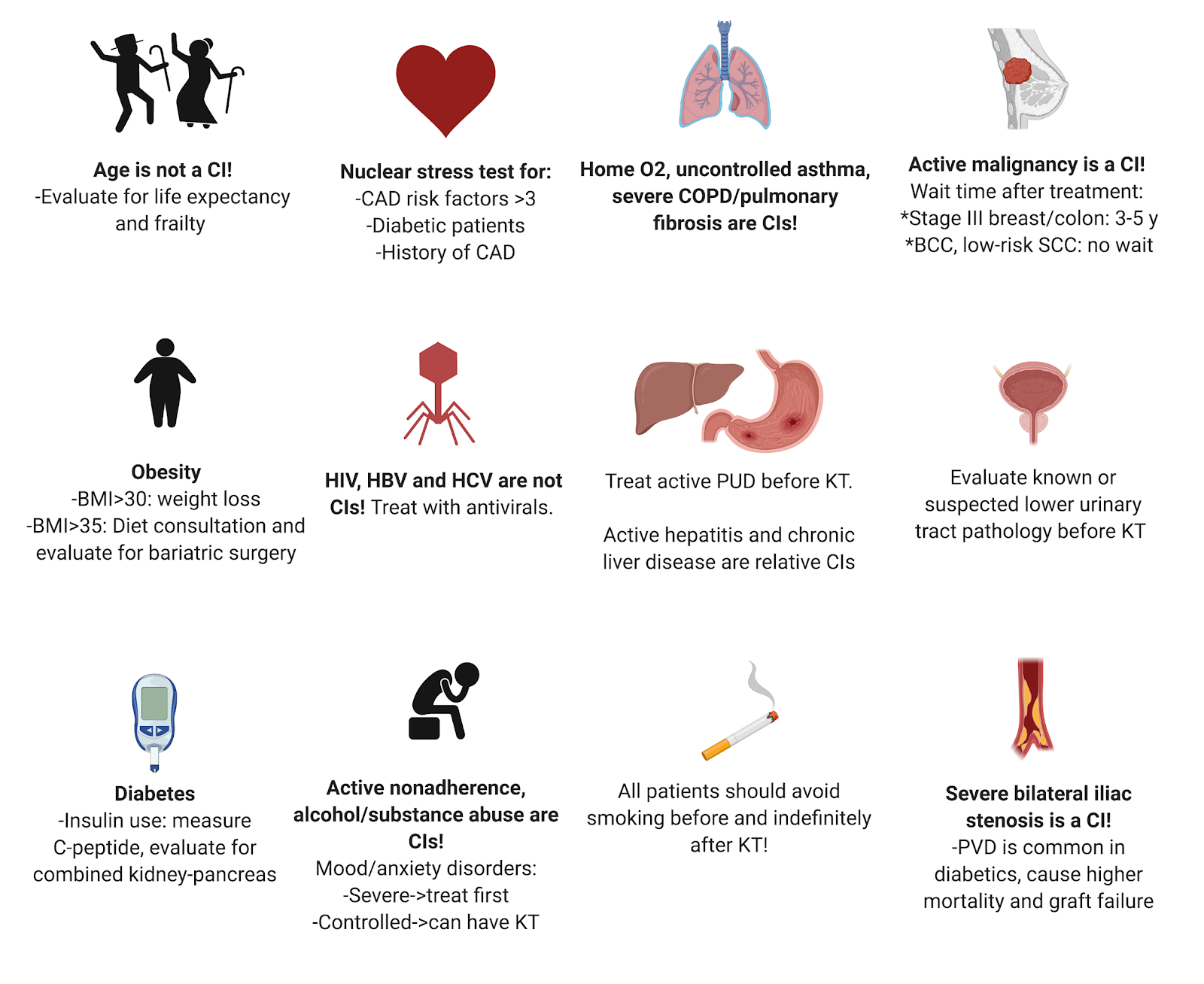
The meticulous evaluation of other organ systems also warrants discussion (the following recommendations are as per the 2020 KDIGO transplantation guidelines). Patients with severe or uncontrolled pulmonary diseases such as severe asthma or home O2 requirement should be excluded from KT. From a metabolic standpoint, insulin requiring diabetic patients should be assessed with C-peptide levels as patients with undetectable or very low levels could be a candidate for combined pancreas and kidney transplantation. Patients with high BMI >30 should be consulted for weight loss, or evaluated for bariatric surgery if BMI>35. Patients with tertiary hyperparathyroidism should undergo parathyroidectomy before proceeding with transplantation for a goal PTH<500. From a gastrointestinal (GI) perspective, patients with active GI disease such as active peptic ulcer disease or active hepatitis should be treated and show improvement prior to KT. Cirrhotic patients should undergo evaluation for combined liver and KT. In consideration of neurological events, patients with a recent episode of stroke or thrombotic microangiopathy should wait at least 6 months before transplantation. Also, patients with risk factors or known peripheral vascular disease should undergo non-invasive imaging with non-contrast abdominal CT for the assessment of the iliac arteries. HBV, HCV, and HIV infections are not contraindications to KT but deserve appropriate antiviral treatment. Patients should also complete their indicated vaccines at least 4 weeks prior to transplant.
Figure 2 summarizes comorbidities that need to be addressed prior to transplantation. It is important to be aware of variation in practices between guidelines and transplant centers.
Post reviewed by: Samira Farouk, Leo Riella, Sam Kant


Hey Raheel, search this site for “transplant immunology and you’ll find a small review on the basics. Also, CJASN has a “renal immunology for the clinician” series that is very in-depth but you can just look at the sections you want. Finally, AJKD has a “core curriculum” section that has a review called “transplant immunology and immunosuppression” from 2015.
I hope these are useful 🙂
Smart review
what about Recipient with Urinary incontinence
Please share if there is any Post regarding Immunological concepts of Renal Transplantation.