Dr Dilushi Wijayaratne, MBBS, MD
Specialist Nephrologist
University of Colombo, Sri Lanka
@Dilushiwijay
The preoperative cardiac evaluation of kidney transplant candidates is a blurry area. Guidelines are variable and clinical practice is frequently reflexive or defensive rather than evidence-based. In this blog we look at some of the issues related to cardiac evaluation of these patients.
Background
Chronic kidney disease (CKD) is a major risk factor for coronary artery disease (CAD). In fact, the presence of albuminuria is itself an independent risk factor. There is a graded association between lower levels of estimated glomerular filtration rate (GFR) and the risks of death and cardiovascular events, which becomes evident at an estimated GFR of less than 60 ml per minute per 1.73 m2. This cardiovascular risk exceeds the risk of progression to end-stage kidney disease. Patients undergoing kidney transplantation are at risk for major adverse cardiac events (MACE) peri- and postoperatively. Moreover, they are exposed to a lifetime of immunosuppressive medications such as steroids and calcineurin inhibitors that are known to accelerate atherosclerosis.
Some of the questions that we hope to answer from cardiac assessment are
- How likely is the patient to have a cardiac event perioperatively?
- Can we prevent a perioperative or long-term adverse cardiac outcome by intervening prior to the kidney transplant? – Of particular relevance as both a cardiac event and an intervention can have a negative impact on the kidney allograft.
- How long is the patient likely to live after a successful surgery? And how does this relate to the utilitarian allocation of scarce organs?
The current guidelines regarding cardiac evaluation of kidney transplant recipients from leading international kidney societies and organizations are summarized in Table 1.
| Whom to screen? | Recommended screening/ intervention | Comments | |
| KDIGO (2020) | Asymptomatic kidney Tx candidates at high risk for CAD or with poor functional capacity | Noninvasive CAD screening. Asymptomatic patients should NOT be revascularized exclusively to reduce perioperative cardiac events | Suggest not excluding candidates with advanced CVD from kidney Tx. |
| ERBP (2013) | Asymptomatic high-risk patients High risk = older age, DM, history of CVD | Standard exercise tolerance test and cardiac ultrasound- If positive or inconclusive ETT do noninvasive stress imaging (myocardial perfusion or dobutamine stress echocardiography) Recommend coronary angiography in kidney Tx candidates with a positive test for cardiac ischemia | Further management according to current cardiovascular guidelines |
| AHA (2012) | All candidates multiple CAD risk factors = 3 or more of DM, prior CVD, >1 y on dialysis, LV hypertrophy, age > 60 y, smoking, HTN, and dyslipidemia) | Echocardiography, noninvasive stress testing may be considered | |
| UKRA (2011) | NO compelling evidence that pre-Tx screening tests for CAD in asymptomatic patients with established kidney failure is effective in preventing future cardiac events or reducing mortality after Tx | Until better evidence emerges, screening tests may be best used to identify high-risk patients for EXCLUSION from the waiting list | |
| AST(2002) | Patients at “high risk” (kidney disease from DM, history of IHD, or 2+ risk factors) | Non invasive stress testing à If positive for CARevascularization before Tx recommended for patients with critical coronary lesions |
The lack of consensus among these bodies reflects a lack of evidence. There is ambiguity about the purpose of screening, what constitutes high-risk for CAD, and whether to intervene on patients with positive stress tests or coronary angiography. Much of the guidance is based on expert opinion.
Let us take a closer look at the data.
First, why screen patients at all?
As discussed above the risk of CAD is increased in patients with CKD. However, these patients may remain asymptomatic, sometimes due to reduced mobility, or may have atypical symptoms such as breathlessness rather than classic angina. The purpose of screening is to pick up patients with asymptomatic CAD so they may be risk stratified and offered optimal medical treatment with or without intervention.
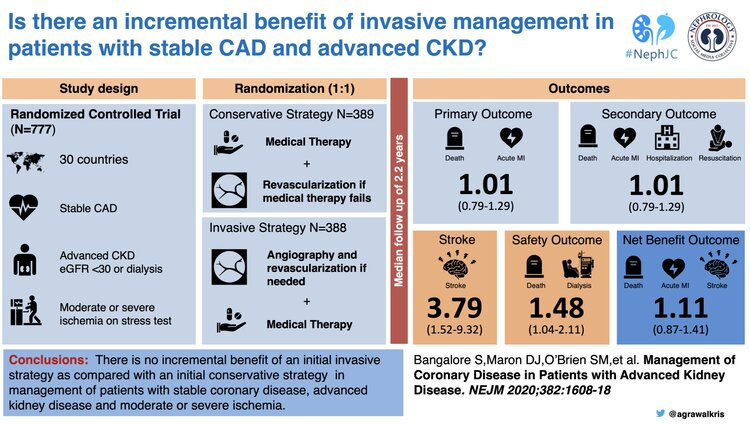
So should we be screening all patients with CKD, regardless of plans for kidney transplantation? This question was addressed in the recently published ISCHEMIA CKD trial which included a cohort of 777 patients with advanced CKD (GFR <30ml/min) who had moderate or severe ischaemia on non-invasive cardiac stress testing and were randomised to either an invasive strategy or optimal medical management. The conclusion was that there was no benefit in an invasive approach vs a conservative approach after screening patients with advanced CKD for CAD, in terms of preventing death or non-fatal myocardial infarction over a median follow up period of 2.2 years. The cohort included patients on dialysis for whom conclusions were similar. Interestingly, only 50% of patients who went on to coronary angiography in the intervention arm proceeded to revascularization; the most common reason being absence of significant obstructive coronary disease! There was a higher risk of stroke and initiation of dialysis in the intervention arm, raising questions on the value of an invasive strategy and the utility of screening asymptomatic patients as a whole.
Are there special considerations to be made for cardiac screening in kidney transplant candidates?
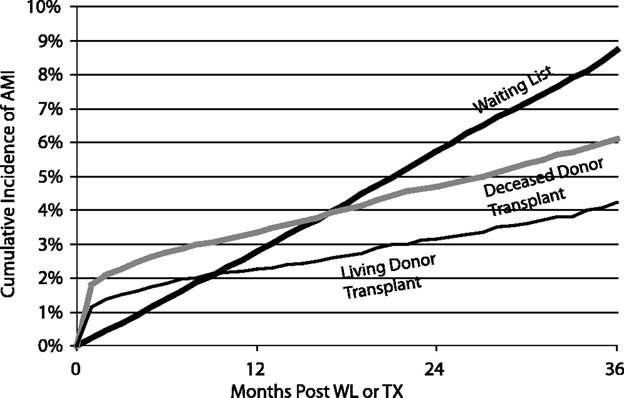
Data reflects an increase in the risk of cardiac events in the immediate postoperative period which is likely to be due to the stress of high-risk vascular surgery- the kidney transplantation (Figure 1). Over long term follow up, the incidence of myocardial infarction (MI) falls in patients who have been transplanted compared to those who remain on the transplant waiting list. The rationale for using a non-invasive stress test lies in its ability to act as a surrogate for the surgery. If inducible ischemia is observed, it may suggest that there is a risk to surgery which might be improved by coronary intervention.
However, screening tests are less sensitive and less specific in the advanced CKD population (Table 2).
| Screening test | Sensitivity | Specificity | Comments |
| Cardiac CT | 96% | 66% | Provides anatomical information. Non-specific medial calcification is common in CKD. Requires exposure to contrast and radiation |
| MPS1,2,3 | 37-80% | 37-73% | MPS involves radiation. Apparent superiority of DSE is lost when lower quality studies are excluded |
| DSE1,2,3,4 | 37-95% | 71-95% |
A positive non-invasive stress test is associated with a poorer prognosis. However, its relationship with significant CAD on coronary angiography is less clear. One explanation for the lower specificity (vs coronary angiography, the gold-standard) may be the higher prevalence of microvascular disease in the CKD population. The lower sensitivities noted in some studies may also reflect the higher burden of non-atherosclerotic cardiac disease in this population. Another point to consider is that tachycardia, increased shear stress and the hypercoagulable state contribute to most acute cardiac events in the postoperative period. Because the nidus for thrombosis is often a noncritical stenosis, preoperative cardiac evaluation before surgery may fail to identify patients at risk for plaque rupture, although control of heart rate may decrease the propensity of plaque rupture regardless of stenosis severity.
Only one RCT, Masnke, Lancet, 1992 has specifically addressed the question of revascularization prior to kidney transplantation in patients with asymptomatic CAD. This study screened 151 kidney transplant candidates with diabetes mellitus using coronary angiography, and 26 of 31 with >75% stenosis in at least one vessel were randomized to revascularization or medical management. Benefit weighted towards revascularization with 2 vs 10 cardiovascular events on follow up in the medically managed group, including 4 deaths due to MI. However, medical management was far below modern standards and included only aspirin and calcium channel blockers, making this very small study only of historical interest.
In the slightly more recent DECREASE V (2007) trial which looked at screening and intervention in the general population prior to major vascular surgery (included 20% of patients with “history of renal failure”) those with 3 or more risk factors who screened positive for extensive cardiac ischemia on non-invasive stress testing were randomized to revascularization or medical management with no difference in all-cause mortality or MI at one year or on longer follow up (median 2.8 years).
Another trial in the general population, the CARP trial, compared revascularization vs medical management for 510 high-risk (risk factors or positive non-invasive stress tests) patients with >70% stenosis of one or more coronary vessels on coronary angiography, prior to elective major vascular surgery. They found no difference in short-term or longer term mortality between groups.
Observational data from kidney transplant recipients is conflicting. Data from a prospective cohort of 222 kidney transplant candidates, published by Patel et al AJT, 2008, showed that high risk patients who had coronary angiography (+/- intervention) had equal survival to those who had had no coronary angiography. A problem with such non-randomized studies is that patients with poor prognostic anatomy on coronary angiography often proceed to intervention, which does not allow us to compare the effect of intervention vs optimal medical management in this group. In a few of these observational studies where patients had been offered but refused revascularization, outcomes had been poorer suggesting there may be a benefit in revascularizing high risk patients, but numbers are often small and factors affecting patient choice may bias results. Furthermore, exclusion from transplantation may deny them the cardiovascular benefit of a kidney transplant.
Thus, evidence for prospective kidney transplant recipients to undergo screening for coronary artery disease is lacking and a randomized trial that addresses this question is necessary. It has been estimated that such a trial would need to recruit 4000 patients and, though not impossible, is likely to be challenging.
Overall benefit from invasive coronary artery intervention is unclear and (if it exists) may be restricted to a very small proportion of patients with high risk anatomy
Does this warrant screening of all patients? And why are we concerned?
Screening takes time, and this leaves patients on the waiting list for longer, allowing them to accrue more cardiac and non-cardiac injury due to poor kidney function and hemodialysis. We know that prognosis is poorer after kidney transplantation for those of a higher dialysis vintage. Screening uses scarce resources which could be diverted to other areas of need. Screening is often inconclusive, resulting in further investigation, further delay and much anxiety. Coronary angiography and cardiac computed tomography (CT) carry a risk of acute kidney injury and exposure to radiation, and intervention carries a small but significant risk of adverse events including stroke and death. The need for dual antiplatelet therapy (DAPT) following certain interventions may delay transplantation further as some surgeons are hesitant to operate on these patients while on DAPT. All this comes at a financial cost to the individual and the health system. Finally, having made it through some of the hoops, some patients may still be denied transplantation based on cardiovascular risk alone.
So where do we stand?
The jury is still out on how best to assess and manage these patients. We know that for a patient with kidney failure the greatest intervention that can improve one’s cardiovascular risk is kidney transplantation (Figure 1). It is often those with the highest cardiovascular risk who stand to achieve the greatest cardiovascular benefit from kidney transplantation. As nephrologists our goal should be to get these patients to the point of kidney transplantation as soon as possible.
Screening and intervention for asymptomatic patients incurs expense and causes delay, is not without risk, and is still without proven benefit. Until a RCT including high risk kidney transplant candidates is undertaken to address this specific question we may not have a definite answer. Unfortunately, habit and tradition are hard to break and cardiovascular screening is firmly entrenched into pre-transplant protocols. It seems that we might serve our patients better by reassessing our guidelines. If we do, perhaps we will find it is time for a change of heart.
Reviewed by Matthew A. Sparks, Amy Yau and Sudha Mannemuddhu