Sriram Sriperumbuduri MD DM DRCPSC
Nephrology Fellow
The Ottawa Hospital, Ottawa Canada
@sriperumbuduris
What are the other methods to overcome prolonged lost dwell times?
- Tidal PD
- Manual drain at the end of the cycler
- CAPD
- Accept a certain level of lost dwell time (ensuring it has no effect on clearance and patient`s sleep)
- Switch to Hemodialysis (HD)
Tidal PD–
Empiric trials of tidal PD are often attempted early in the clinical course, while dealing with PD catheter dysfunction. To understand the concept of tidal PD, review the following pattern of drainage (Figure 10).
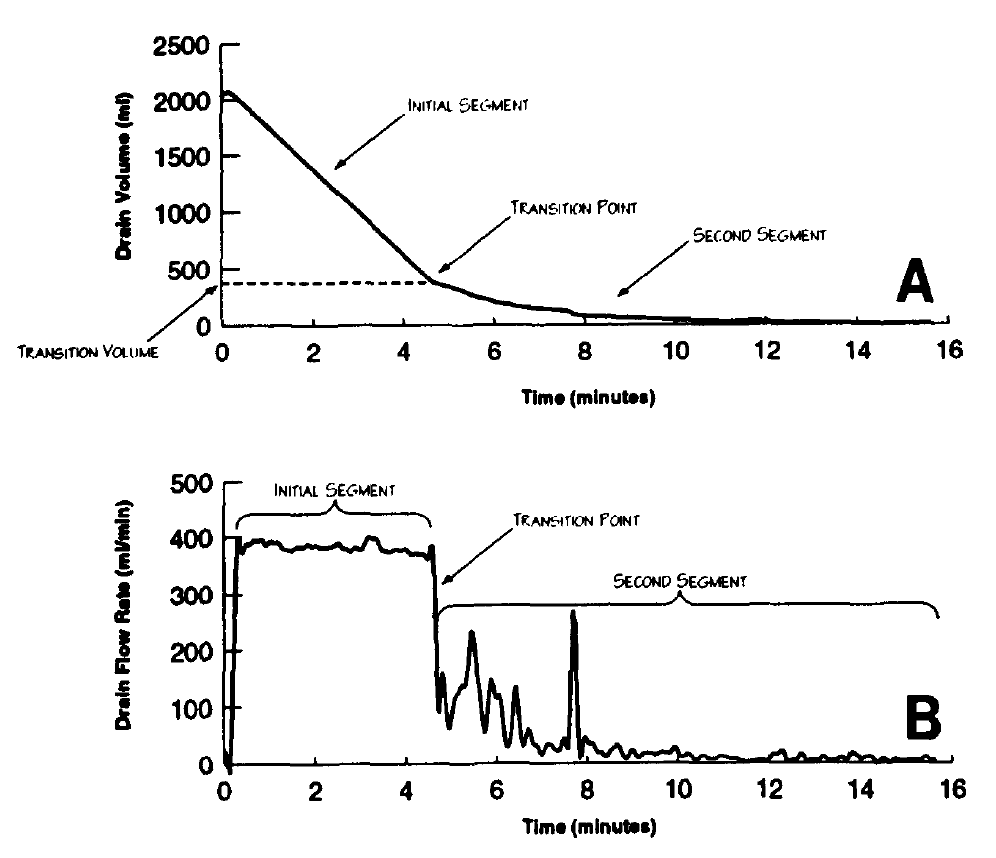
In the above diagram, figure A shows that the initial part of the outflow is very rapid with a steep curve, then at a certain point (Transition point), the outflow slows down suddenly and the slope of the curve becomes less steep. Of note, 75% of the drainage occurs within the first part of the drainage (about 5 minutes in the diagram) and 25 % of the drainage happens over 5-6 minutes. Part B describes the same phenomenon in terms of flow rates.
With tidal PD, we attempt to start the next dwell prior to the transition point. Furthermore, some etiologies of catheter dysfunction may be alleviated by maintaining dialysate in the peritoneum, preventing catheter kinking or omental wrapping during drainage. Though we cannot precisely pinpoint the transition point with most of the available cyclers (with the exception of AMIA system- Baxter), the percent of Tidal programme is usually set to 80-85 % arbitrarily and then lowered depending on the clinical response. However this number could vary depending on the experience of a particular center. Previous studies have described the use of upto 50 % tidal in significantly decreasing the incidence of low drain volume alarms on the cycler.

Tidal PD is also efficacious in decreasing the drain pain associated with PD, as described in a previous article from RFN.
Let’s look at a case study highlighting some of the problems I discussed in the above paragraphs.
A 75-year-old man with kidney failure due to diabetic nephropathy with an eGFR of 8 ml/min/1.73m2, was initiated on NIPD (non-tidal) after externalisation of a buried PD catheter. Each cycle had a fill volume of 2 liters and 4 exchanges were done overnight over 8 hours. Following initiation of PD, he had good inflow but poor outflow through the catheter. Empiric laxative therapy was attempted without benefit. Abdominal x-ray ruled out constipation but showed a displaced PD catheter tip. Fluoroscopic manipulation was performed and the catheter tip was repositioned into the pelvis. Despite that, the patient continued to have persistent lost dwell times. Repeat abdominal x-ray ruled out catheter displacement and kinking. He was switched to Tidal PD with 85% volumes. Even with the tidal prescription, lost dwell times continued to be high (up to 90 minutes every night with alarms). At this point, we noted that his net UF was -250 ml to -350 ml, indicating that he was reabsorbing fluid. Peritoneal equilibration test (PET) showed that he was a high average transporter. Thus, we decided to increase the number of cycles from 4 to 5, in order to shorten the dwell times on the cycleras he was a high average transporter. This decreased the lost dwell time to 30-60 minutes per night. Next we changed the tidal to 80% with further reduction in the lost dwell time. This illustrates that more than one problem could exist in the same patient which needs to be addressed.
When encountering PD catheter dysfunction, the following algorithm can be followed.
Table 3: Table showing the sequence of steps to be followed while managing PD catheters with inflow and outflow problems
| Order of steps to be followed | Outflow Problem | Inflow Problem |
| Rule out constipation and other causes of compression of external part of the PD catheter | Vigorous push/ pull through the PD catheter with a 30 cc syringe | |
| Heparin added to the bags | Abdominal X-ray to assess tip migration/ tPA lock | |
| If there is catheter migration, fluoroscopic manipulation → if it fails, laparoscopic manipulation | If there is catheter migration, fluoroscopic manipulation → if it fails, laparoscopic manipulation | |
| After ruling out catheter migration → Initiate tidal PD 80% to 85%. In some cases, tidal PD is initiated before ruling out catheter migration. | Removal/ reinsertion of PD catheter | |
| If catheter migration is ruled out and outflow problems persist with Tidal PD, fluoroscopic manipulation to clear any debris or fibrin in the lumen of the catheter and free adhesions | Switch to HD | |
| -Increase the tidal- 70-75% or even lower-Assess the transporter status- -High or high average needs shorter dwell times-Manual drain at the end of cycler-CAPD-Switch to HD |
Prevention of PD catheter dysfunction–
Some of the preventive measures to avoid PD catheter dysfunction include
- Insertion of PD catheter into the peritoneal cavity under direct visualisation
- Loose tacking of the intraperitoneal portion to the peritoneum of the anterior abdominal wall to prevent movement out of the pelvis and
- Fashioning the intraperitoneal portion of the catheter to an appropriate length for insertion into either the pouch of Douglas or rectovesical pouch.
I thank my teachers and the nurses in the Home Dialysis Unit at the Ottawa hospital for helping me understand the concepts of cycler and the PD cycles.

