Brian Rifkin, MD
Hattiesburg Clinic
ASDIN Education Committee
KDOQI Clinical Practice Guideline for Vascular Access: 2019 Update (ajkd.org)
Introduction
Dialysis access planning and placement are cornerstones in the timely initiation of dialysis therapy. Strategies from “Fistula First” to “Catheter Last” have attempted to guide nephrologists and CKD patients to the optimum dialysis access entry point. Unfortunately, like most medical decision making, there is often not a simple one-size-fits-all answer for the ideal dialysis access. In fact, in this recent 2019 KDOQI clinical practice guideline, the focus is primarily on patient shared decision making with plans that are regularly reviewed, updated, and documented. Physicians should focus more on “the right access, in the right patient at the right time”.
What was wrong with “Fistula First”?
Vascular access remains a significant challenge for patients with ESKD. A patient-centered approach to hemodialysis vascular access that considers multiple aspects of a patient’s needs and eligibility is a superior strategy for dialysis access decision making. Some patients, due to poor vasculature or short life expectancy, may not be appropriate candidates for fistula creation. It is best to be creative in thinking about how to prepare for, create, and preserve dialysis access. It is equally important to be proactive in planning for the protection, creation, and preservation of the next vascular access, long before the current one fails. This chain of careful consideration of modalities and dialysis access lifelines, as it pertains to the individuals’ needs and preferences, is the essence of the ESKD Life-Plan.
What exactly is an ESKD Life-Plan?
The ESKD Life-Plan is a strategy for living with ESKD, ideally made together by the patient and the CKD management team. For the purposes of dialysis access this team should include but is not limited to a nephrologist, surgeon, radiologist, nurse, patient family member, or other supporter. The ESKD Life-Plan is a strategy that should start in the predialysis period and maximize ESKD modality choices. Life-Plans should specifically consider the patient’s current medical situation, current and future life goals, preferences, social support, functional status, and logistics.
Who needs consideration for an ESKD Life-Plan?
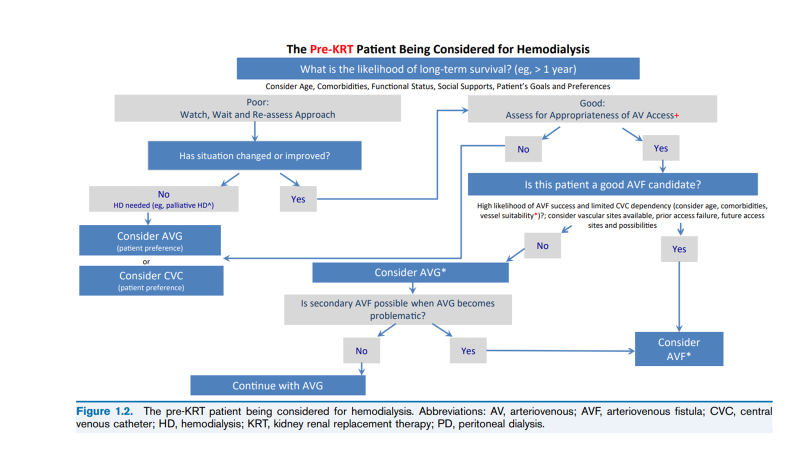
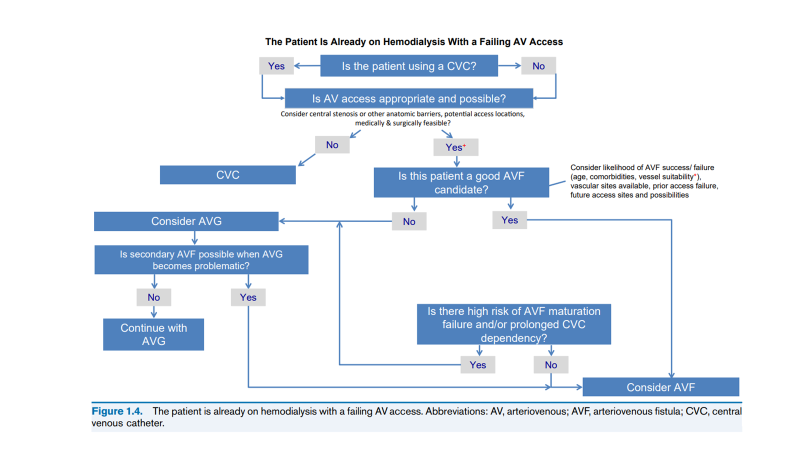
All patients with progressive CKD or on dialysis need an ESKD Life-Plan. Patients may require a new dialysis AV access for multiple reasons. No decision about a single vascular access creation or placement should be made independent of the patient’s overall ESKD Life-Plan. The Life-Plan may need to be altered as the patient’s clinical situation changes. Below are several algorithms discussing patients with ESKD and dialysis catheters, patients with ESKD and failing AV access, patients changing modalities (PD to HD), and patients with failing kidney transplants
(see KDOQI guideline link for additional algorithms).
Is an ESKD Life-Plan a one time discussion?
An ESKD Life-Plan is an evolving strategy. Kidney replacement modality and dialysis access short- and long-term plans should be discussed on a regular basis. The frequency of re-evaluation depends on the patient’s circumstances, but a minimum of yearly is recommended.
Are there areas of dialysis access planning still under evaluation?
Yes, ESKD Life-Plan strategies are still being evaluated for key outcomes including:
- Patient satisfaction with the dialysis access, using a validated instrument
- Rate of unnecessary dialysis access creations/placements
- Rate of vascular access procedures
- Rate of vascular access infections
- Rate of vascular access–related hospitalizations
- Patient burden, which may include all of the above component
Conclusion
Forming a comprehensive plan in conjunction with the patient’s treatment and life goals is the objective of individualizing dialysis access planning and maintenance. Once an access has been placed further discussions should hinge on contingency plans for anticipated problems and a succession plan should the access ultimately fail. Plans need to be updated regularly given that dialysis patients face many obstacles and setbacks that may change their treatment goals. CVC use is still ubiquitous, and every catheter observed dysfunction is an opportunity to engage with patients in discussions about a potentially more appropriate permanent vascular access. Changes in modality due to a failing transplant or ultrafiltration failure with peritoneal dialysis should be met with a detailed discussion of access options in a focused clinical evaluation. ESKD Life-Plans are an opportunity for patients and CKD treatment teams to come to a mutually agreeable strategy that will provide for the best clinical care.
Post edited by: Matt Sparks, MD


nice presentation thanks