Kavitha Ramaswamy, MD
NSMC intern 2022
Sodium Glucose Cotransporter 2 (SGLT2) inhibitors have become the standard of care for primary care, nephrology, cardiology and endocrinology. It is imperative to know how they work and specifically side effects in order to maximize use and minimize harm.
SGLT2 inhibitors reduce the absorption of glucose and sodium at proximal convoluted tubule (PCT) by blocking SGLT2 cotransporters. The net increase in sodium delivery to the thick ascending limb (TAL) activates the tubuloglomerular feedback mechanism which causes afferent arteriole vasoconstriction, resulting in decreased glomerular pressure. Other mechanisms have also been hypothesized such as improved metabolic function. Various randomized clinical trials have demonstrated benefits in all cause cardiovascular mortality in patients with heart failure and kidney disease.
Among the many other purported benefits:
- Systolic blood pressure (SBP) reduction of up to 4 mm Hg which has been attributed to its natriuretic effect.
- They also reduce hepcidin levels, improving erythropoiesis and anemia.
- The ability to reduce weight is also consistently observed in these patients.
- Osmotic diuresis
- Increased serum magnesium
- Reduction in inflammation
With all these wonderful effects, we also have to be vigilant of the potential side effects. Let’s review the side effects and their management.
Volume depletion/dehydration: SGLT2 inhibitors may contribute to volume depletion due to the natriuretic properties. In the CANVAS study, volume depletion was more common in the canagliflozin vs placebo (26 vs 18.5 events per 1000 person-years; P=0.009). In patients who are not volume overloaded and on diuretics, one can consider holding or reducing the diuretic dose when starting an SGLT2 inhibitor to avoid hypovolemia. In patients with volume overload when initiating SGLT2 inhibitors, the diuretic ability is often enhanced.
Multiple studies show an acute reduction in eGFR within the first month of therapy likely related to tubuloglomerular feedback which is not kidney injury. This is also confounded by the presence of other risk factors such as advanced age and concomitant use of medications such as renin-angiotensin-aldosterone system inhibitors and diuretics. In these cases, SGLT2 inhibitors should not be discontinued given long term benefit. SGLT2 inhibitors reduced risk of progression of chronic kidney disease based on the EMPA-REG and CANVAS trials with kidney disease defined by loss of kidney function, eGFR decline, progression or worsening of albuminuria, new ESKD, death from renal causes and/or a renal outcome compared with placebo.
Although SGLT2 inhibitors may impact measured kidney function, a systematic review and meta analysis done by Jan Menne et al showed reduction in occurrence of AKI in patients with diabetes mellitus on SGLT2 inhibitors.
Accurate evaluation of volume status and screening for other nephrotoxic medications is essential before starting SGLT2 inhibitors. FDA recommends monitoring renal function before and after drug initiation especially if patients are already on RAAS inhibitors, diuretics, and chronic NSAIDS.
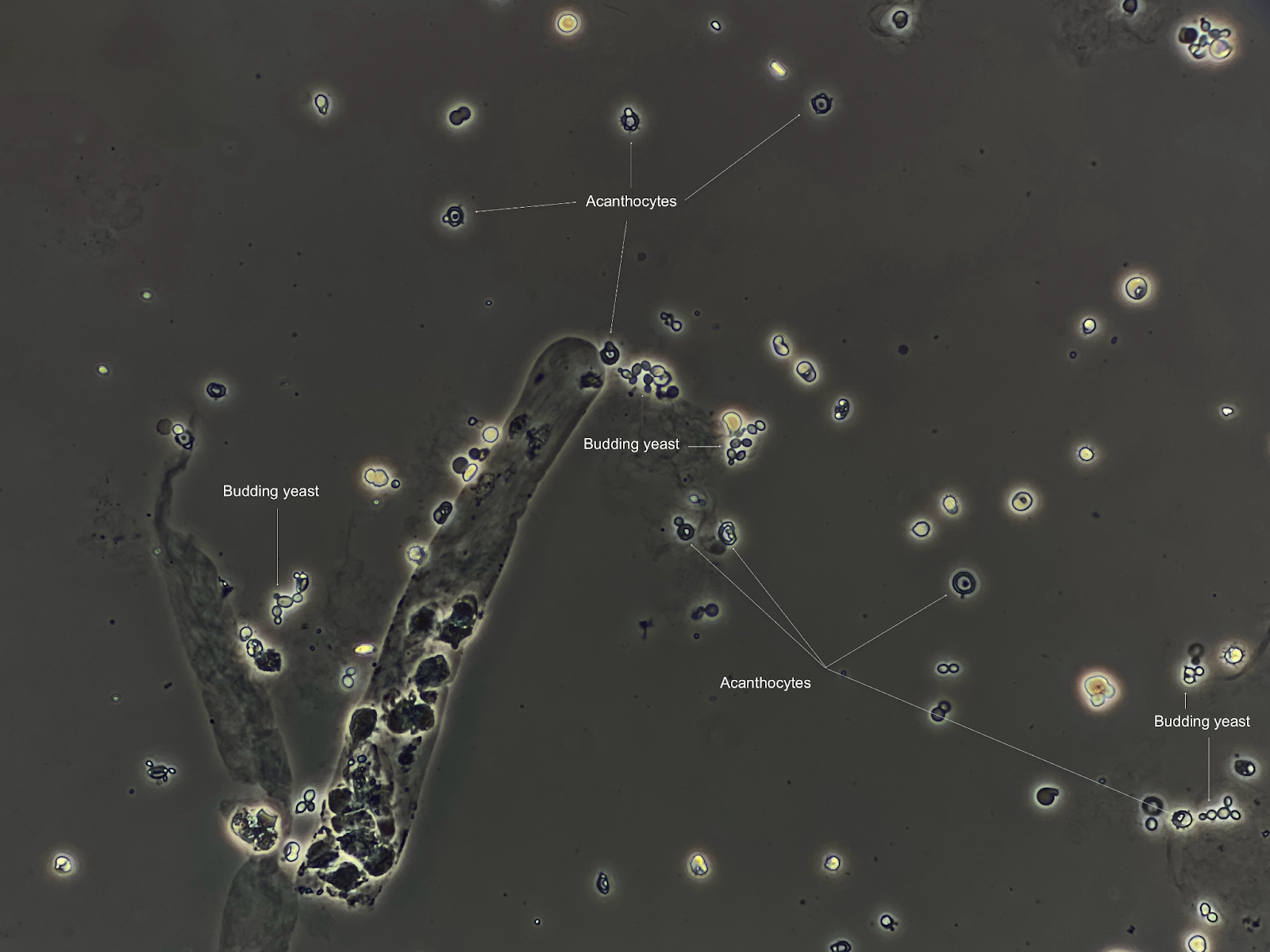
Genital mycotic infections: Genital mycotic infection occurred more frequently in participants treated with empagliflozin (3.5 versus 0.9/100 patient-years). Patients with diabetes and CKD are at higher risk of infections due to their decreased immunity and altered genital microflora. Several studies have shown increased risk of genital mycotic infections but there have not been any data associating SGLT2 inhibitors with increased risk of urinary tract infections. Patients need to be educated about perineal hygiene, as well as symptom monitoring in order to mitigate the risk of genito-urinary infections. In rare scenarios, Fournier gangrene has been seen to occur in patients who are on SGLT2 inhibitors which may lead to life threatening complications. FDA had identified 55 cases of Fournier gangrene in patients receiving SGLT2 inhibitors between 1 March 2013 and 31 January 2019.
Decrease in Blood pressure: SGLT2 inhibitors lower SBP by 4-10 mm Hg. Increased natriuresis leads to decreased blood pressure (BP) which is helpful in people with hypertension but there are concerns of excessive BP reduction causing orthostasis and dizziness. They should be avoided in hypotensive and hypovolemic patients. Patients should be advised to monitor home BP after initiation. In the SGLT2 inhibitors cardiovascular and kidney trials, patients were on a maximum tolerated dose of RAAS blockers before starting on them.
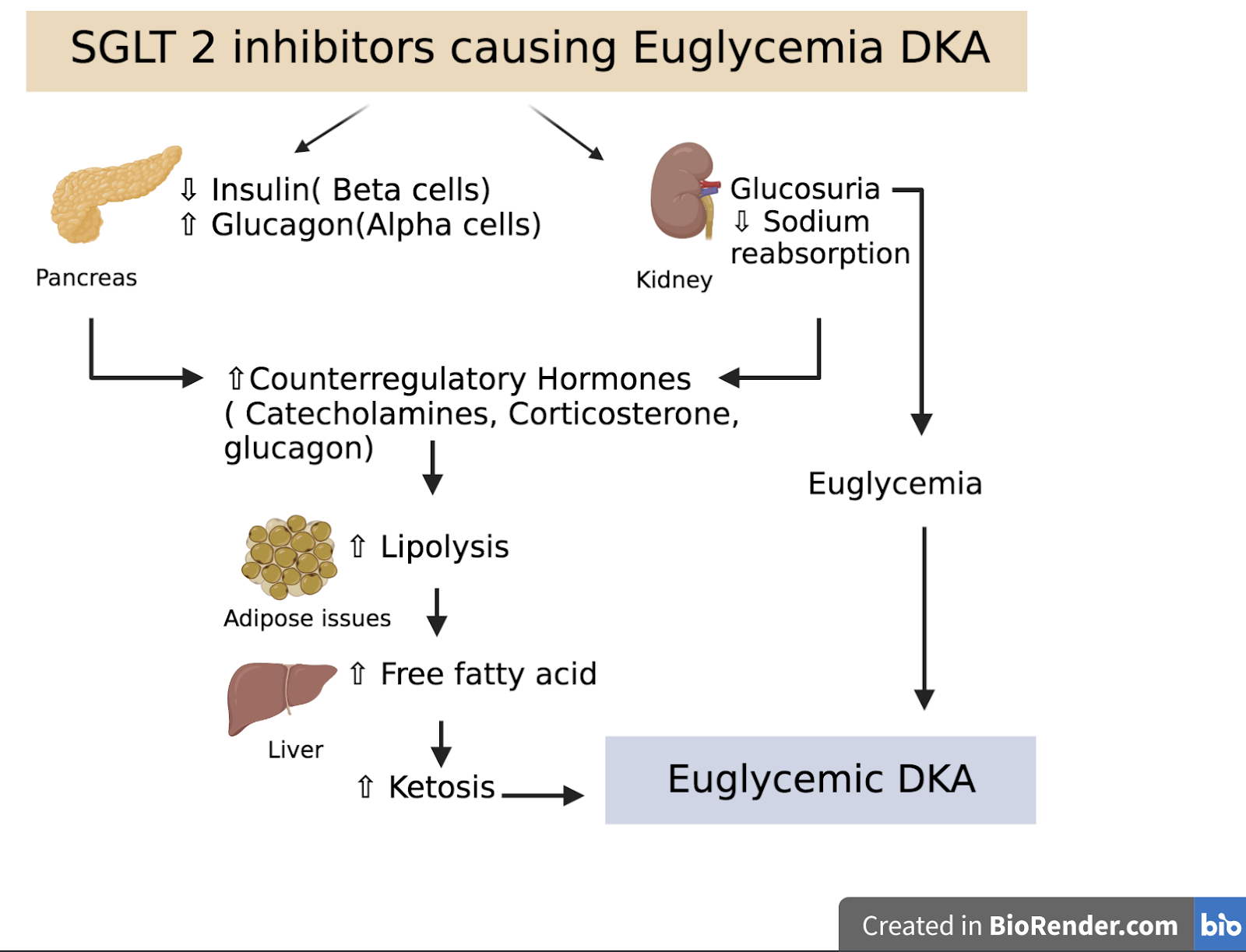
Euglycemic ketoacidosis: Euglycemic DKA (EDKA) is defined as pH less than 7.3, or serum bicarbonate less than 18 with near normal plasma glucose. DKA associated with SGLT2 inhibitors has rates from 0.16-0.76 events per 1000 patient-years in patients with type 2 diabetes mellitus. SGLT2 inhibitors increase the risk of DKA in type 2 diabetics by 7 fold. Overall incidence of DKA in T2D with SGLT2 inhibitors use is 0.1%.
The mechanism is still unclear but thought to be due to decreased insulin and increased counter regulatory hormones leading to shift of glucose metabolism to fat metabolism causing stimulation of ketogenesis. There is an added mechanism of increased renal reabsorption of ketones leading to less ketonuria.
The diagnosis is confirmed with measurement of beta hydroxybutyrate level in blood and acidemia. The predominant ketone body in DKA is beta-hydroxybutyrate, so measuring urine ketones on dipstick ( which assesses acetoacetate) may be deceiving. Once diagnosed, the SGLT2 inhibitor should be stopped immediately and IV fluids and insulin should be administered. Fluid resuscitation is the main form of treatment as patients are usually dehydrated. After volume expansion, a combination of dextrose and insulin infusions may need to be continued until the acidosis resolves. Because of concerns about ketoacidosis, SGLT2 inhibitors are currently not recommended in Type 1 DM or autoimmune forms of diabetes (ie latent autoimmune diabetes in adults (LADA).
Lower limb amputation: Amputation is a very rare adverse effect of SGLT2 inhibitors. The CANVAS trial showed approximately 2-fold increased risk of lower limb amputation in the canagliflozin arm vs placebo (rates were 6.30 vs 3.37 per 1000 participant-years with canagliflozin vs placebo). Meta-analyses of randomized controlled studies have not confirmed these findings. Interestingly, a recent study by Lin et al suggests that the increased risk of LLA associated with SGLT2 inhibitors could be mediated by diuretic induced hypovolemia, leading to distal hypoperfusion, ischemia, necrosis and eventually amputations. However, it must be noted that this is still controversial. Importantly, the FDA removed the black box warning for the risk of amputations with canagliflozin in late August of 2020. However, the risk is still described in the warning and precautions section of the prescribing information. Physicians should be aware and pay close attention to the development of peripheral wounds or ulcers.
Bone Fracture: An analysis of data on canagliflozin use from nine randomized controlled trials, including CANVAS, showed a higher incidence of fracture with canagliflozin (2.7%) vs comparators (1.9%) in the overall population. Given this, FDA has warned but not affirmingly concluded about increased risk of bone fractures with the use of canagliflozin. Possible mechanisms include increased risk of falls from volume depletion/ hypoglycemia and decrease in bone quality through weight loss, increased bone turnover, and disturbed calcium-phosphate balance. Patients with CKD are more susceptible to changes in bone quality due to pre-existing bone mineral disorder.
A recent study by Cowan et al. compared fracture risk in patients on SGLT2 inhibitors (n=38994) and DPP4 inhibitors (n=37449) and concluded that SGLT2 inhibitors were not associated with higher risk of fractures. There was no significant difference in fracture incidence at 185 and 356 days. More studies are needed to ascertain the potential risk for fractures related to SGLT2 inhibitors use. Till then, we need to be aware of these effects and pay closer attention to the bone mineral disease balance in this population.
Bladder cancer: Across 22 clinical studies, newly diagnosed cases of bladder cancer was reported in 10/6045 patients (0.17%) treated with dapagliflozin and 1/3512(0.03%) treated with placebo. Although this was seen in the earlier studies, subsequent studies have not been able to relate the side effect. Given the short-term design of the RCTs, long term effects on cancer still remain uncertain. Long term studies and surveillance studies are warranted. Hence, SGLT2 inhibitors should be used with caution in patients with a history of bladder cancer or patients with unexplained hematuria and risk factors for malignancy.
A comprehensive table of side effects of SGLT2 inhibitors are listed in Renal Fellow Network of various clinical trials but despite the above mentioned side effects in SGLT2 inhibitors, it is essential that they are started early in eligible patients to maximize long term cardiorenal benefits.
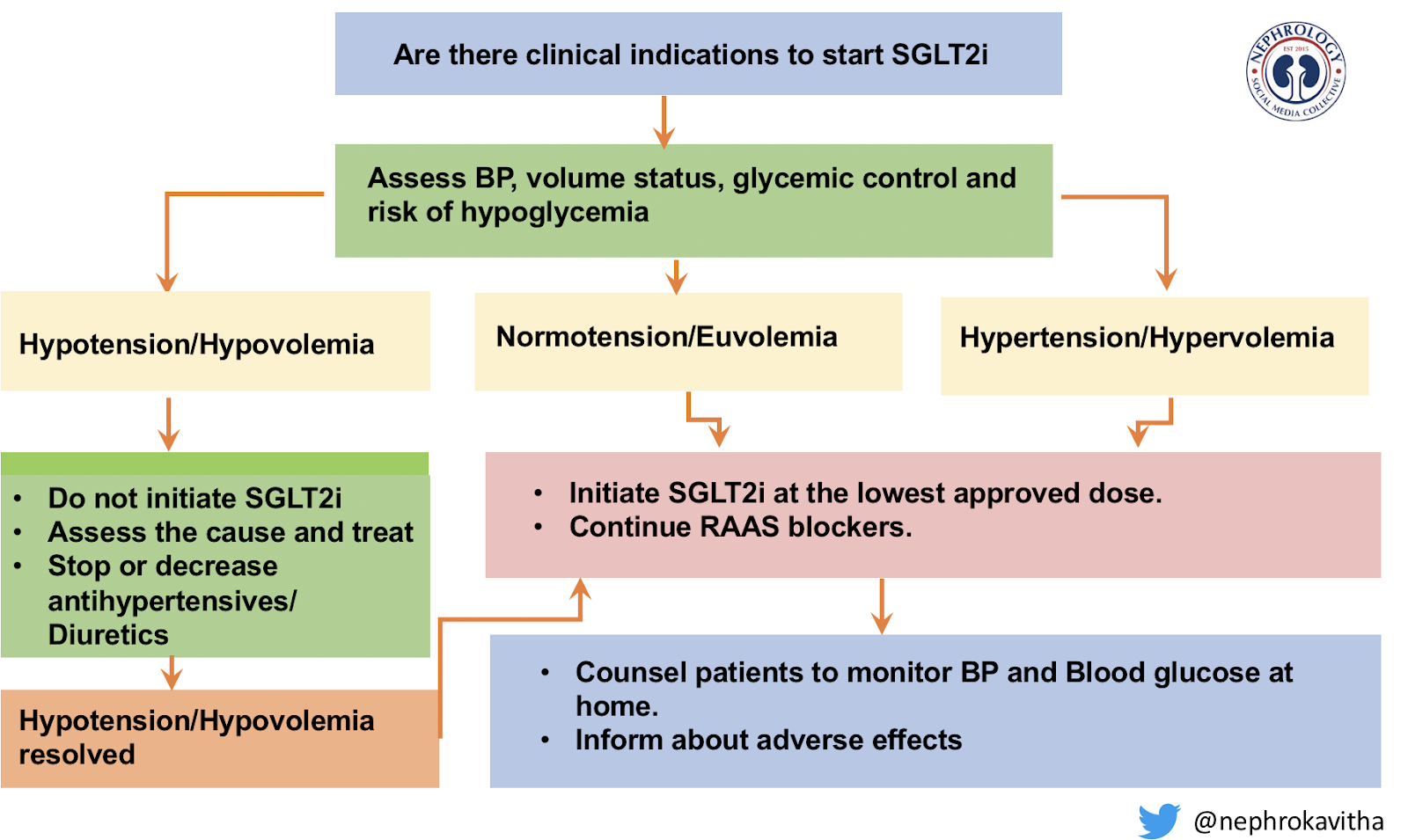
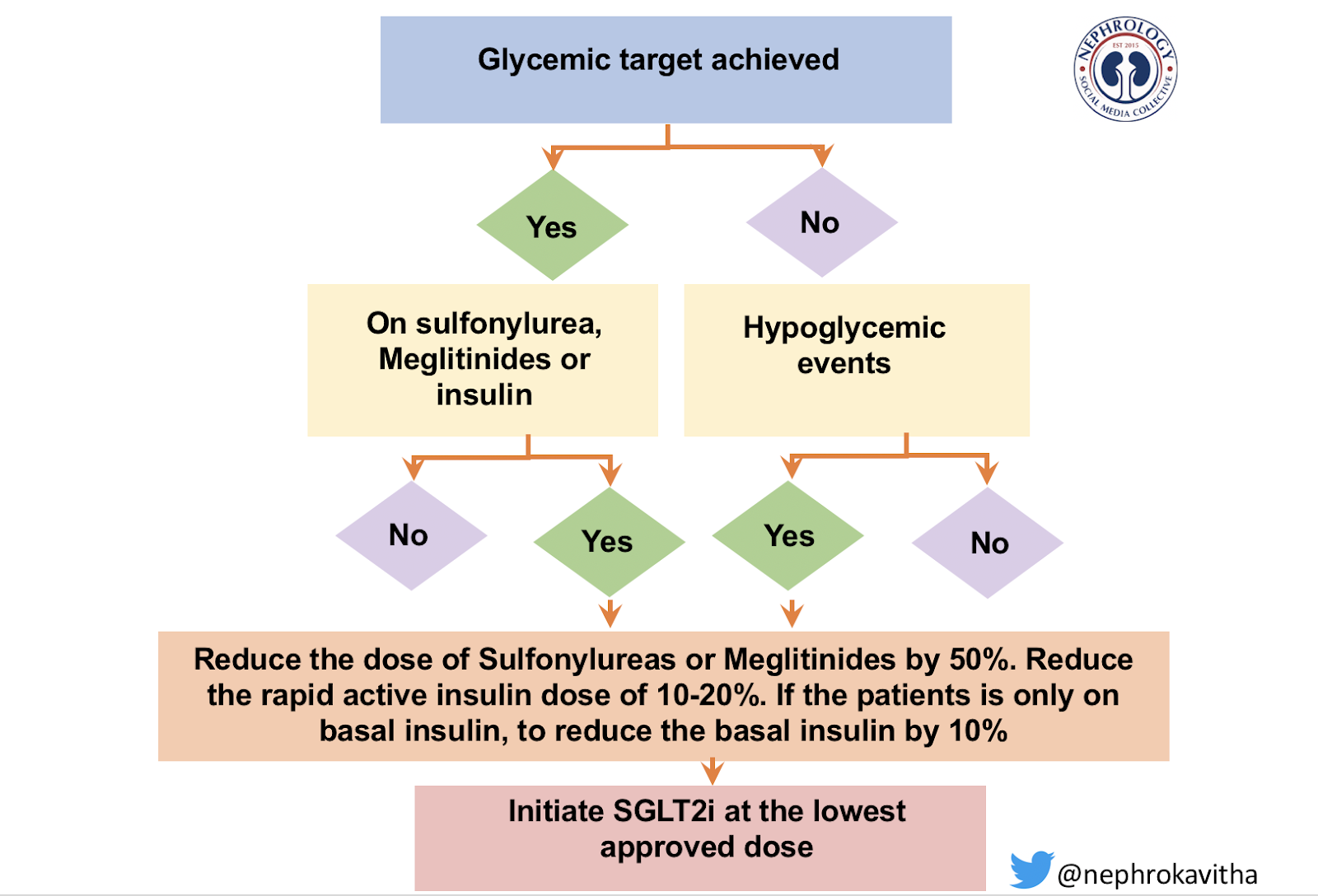
Here is one proposed algorithm for prescribing SGLT2 inhibitors.
In conclusion, SGLT2 inhibitors are a relatively new class of drugs and long term studies are required for their safety. Clinicians should be aware of common side effects like hypotension, rise in creatinine and euglycemic ketoacidosis to help counsel patients and close follow up and early management.
Post reviewed by Matthew A. Sparks, MD