
Avinash Rao Ullur, MD
DrNB (Nephrology), FASN, CHS
Clinical Fellow in Onconephrology
The University of Toronto, Canada
Aisha Shaikh, MD
Associate Attending, Renal Division
Department of Medicine
Memorial Sloan Kettering Cancer Center
Acknowledgements: This post is part of a collaboration between The Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. For more information about the ASDIN mission or membership, click here. Special thanks to the ASDIN Fellows Education Committee for their support on this project.
Coronary angiography and percutaneous coronary intervention are minimally invasive procedures performed to improve coronary blood flow. These procedures can cause periprocedural bleeding which can increase patient mortality. In recent years, the radial artery has become the preferred arterial site of access for performing coronary procedures. Compared to the conventional femoral artery access, radial artery access lowers risk of bleeding and vascular complications. Furthermore, radial artery access enables early patient ambulation, reduces length of stay and improves patient comfort. In the conventional transradial artery approach the radial artery is accessed proximal to the styloid process of the radius bone whereas in the distal radial artery approach the radial artery is accessed distal to the styloid process of the radius bone (Figure 1). The major disadvantage of radial artery access for cardiac catheterization is the possibility of radial artery occlusion. Early studies demonstrated in procedures utilizing the transradial artery approach there was a radial artery occlusion rate of 7.5% at 24-hours and 5.5% at 30-days. It is worth noting that spontaneous recanalization of the radial artery within 1-3 months following radial artery access has been reported. Furthermore, resolution of arterial occlusion with anticoagulation and angioplasty has also been described. Therefore, in the setting of radial artery occlusion, a follow-up assessment of the radial artery must be done as part of AVF creation planning. Potential risk factors for radial artery occlusion are summarized in Table 1.
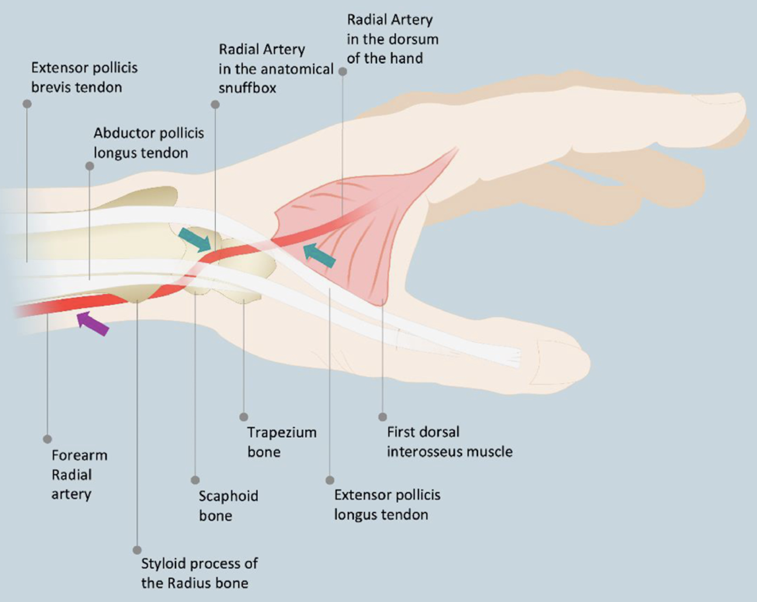
Figure 1. Anatomical landmarks of conventional transradial artery access and distal radial access. Violet arrow points to conventional transradial access puncture site at wrist level; turquoise arrows point to the distal radial access punctures sites in the anatomical snuffbox and in the dorsum of the hand.
Table 1: Potential Risk Factors for Radial Artery Occlusion Following Radial Artery Access for Cardiac Catheterization
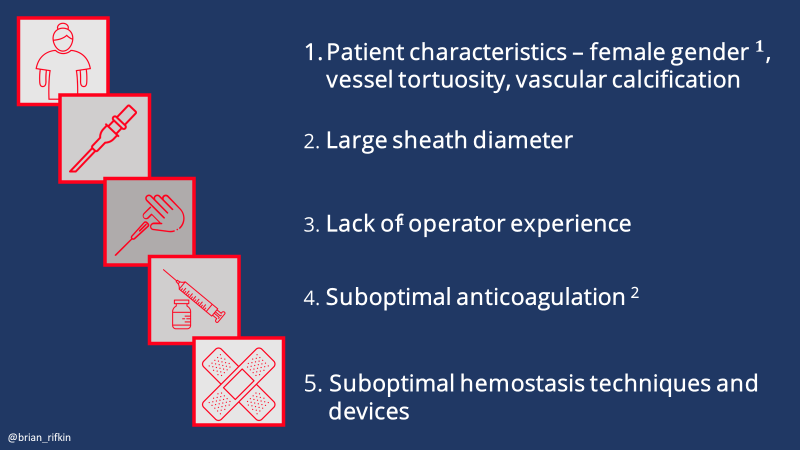
1 Gender differences in the distal radial artery diameter for the snuffbox approach
Patients with CKD frequently undergo cardiac catheterizations and are at high risk for periprocedural bleeding with the conventional femoral approach for arterial access. Therefore, it makes intuitive sense to use radial artery access for cardiac catheterization in patients with CKD. However, interventionalists tend to avoid cardiac catheterization via the radial artery in patients with CKD to prevent radial artery occlusion and to preserve the radial artery for future arteriovenous fistula (AVF) creation. In general, radial artery occlusion does not result in symptoms of hand ischemia due to presence of dual circulation and extensive collateralization of the interosseous arteries in the hand. Let’s examine the data on radial artery access for cardiac catheterization in patients with CKD.
In 2018, Kuno et al prospectively assessed 88 patients on dialysis who underwent cardiac catheterization by either radial artery access (n=62) or femoral artery access (n=26). Radial artery access was limited to the arm contralateral to any functioning AVF. Allen’s test (Figure 2) was not routinely performed as it has not shown to predict development of ischemic symptoms. Sheaths from 4Fr to 7Fr were used for arterial access, with 6Fr being most common (71%). Following radial artery access, heparin and nitroglycerin were administered intra-arterially to prevent arterial spasm, and additional heparin was administered if PCI was performed. Hemostasis at the arterial puncture site was obtained using the Bleedsafe device (Figure 3) and prophylactic ulnar artery compression was applied. The presence of radial artery occlusion was assessed by Barbeau’s test. This study demonstrated no difference in the in-hospital or 30-day mortality between the radial and the femoral approach groups. Puncture site bleeding occurred in one patient (3.8%) in the femoral group compared to 0% in the radial group (P=0.12). A puncture site hematoma was reported in one patient (1.6%) in the radial group. The procedure success rate was 98.4% in the radial group with only one patient requiring crossover to the femoral group due to radial artery spasm. Radial artery occlusion occurred in 4 patients (6.5%) at 24-hours post-procedure and radial artery occlusion was confirmed at 30-days post-procedure. None of the 4 patients with radial artery occlusion reported symptoms of hand ischemia. In the 4 patients with radial artery occlusion, either a 6Fr or a 7Fr sheath was used for arterial access.
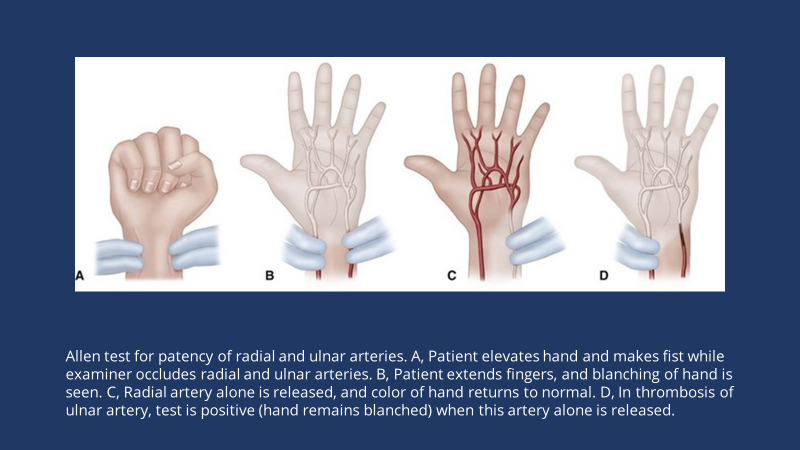
Figure 2 Allen Test

Figure 3 Bleedsafe devices

Video: Barbeau Test For Radial Artery Access
In another prospective cohort study, Kuno et al assessed 306 patients with CKD stages 4 and 5 (including patients on dialysis) who underwent coronary angiography and/or PCI by either radial access (n=114) or femoral access (n=192). Patients in the radial artery group were older (73.3 years vs. 70 years) but had fewer comorbidities such as diabetes mellitus, end stage kidney disease and 3-vessel coronary artery disease compared to patients in the femoral group. Among patients on dialysis, 33 patients underwent cardiac catheterization by radial access versus 123 patients by femoral access. In the radial artery group, 6Fr sheaths were used in 85% patients and 7Fr sheaths were used in 13% patients.
- The composite outcome of in-hospital bleeding and in-hospital death following PCI was lower in the radial group compared to the femoral group (11.5% vs. 2.6%, p=0.006).
- Crossover from the radial to the femoral group occurred in 3 patients (2.6%).
- Among patients on dialysis, radial artery occlusion occurred in 3 out of 33 patients (9.1%) at 24-hours and was reconfirmed at 30-days following cardiac catheterization.
- None of the patients with radial artery occlusion reported symptoms of hand ischemia.
Due to the high rate of arterial occlusion observed with the conventional radial artery access, distal radial artery access (also known as the snuffbox approach) has emerged as an alternative cannulation site for cardiac catheterization. The advantage of distal radial artery access is that it carries a lower risk of radial artery occlusion, and it may preserve the proximal radial artery for future AVF creation.The DAPRAO (Distal Radial Approach to Prevent Radial Artery Occlusion) study was a randomized, prospective, single center study, that compared the rate of proximal radial artery occlusion in patients undergoing coronary angiography or PCI by either the distal radial artery access or conventional radial artery access. A total of 282 patients were randomized to either the distal group (n=140) or to the conventional radial artery (n=142) group. The mean age of the patients in this study was 62 years and only 5% of patients had CKD. A 6Fr sheath was used in 93% of patients in the conventional radial artery group and in 88.5% patients in the distal radial artery group.
- The rate of proximal radial artery occlusion was significantly lower in the distal artery access group compared to the conventional radial artery group at 24-hours and 30-days following cardiac catheterization (0.7% vs 8.4% at 24-hours and 0.7% vs 5.6% at 30-days).
- However, the rate of crossover to the opposite arm was more frequent in the distal radial artery group than in the traditional radial artery group (19 patients vs. 1 patient).
The findings of this study suggest that distal radial artery access was better at preserving the patency of the proximal radial artery than conventional radial artery access, but had a higher crossover rate
The DAPRAO study was followed by the DISCO RADIAL (Distal versus Conventional Radial Access) trial; a prospective, international, multicenter, open-label, randomized controlled trial in which patients undergoing coronary angiography or PCI were either randomized to distal radial artery access (n=650) or conventional radial artery access approach (n=657). The operators in the study were very experienced and had performed a minimum of 100 procedures utilizing distal radial artery access. In this trial, a standardized 6Fr Glidesheath Slender (Terumo sheath) was used in all patients. All patients received 5000 units of IV heparin with additional doses of heparin as needed to maintain an activated clotting time of 250-300 seconds. Verapamil 5 mg and/or nitroglycerin 100-200 mg was administered to prevent arterial spasm. The mean age of the patients was 68 years, and the mean creatinine was 1.0 mg/dL.
- Crossover rates were significantly higher in the distal radial group (7.4% vs 3.5%, p=0.002). The majority of crossover events in the distal radial group and were switched to traditional radial access while the majority of crossover in traditional radial artery access switched to either the opposite arm or to femoral artery access.
- Forearm radial artery occlusion occurred in 6 patients in the traditional radial artery group and in 2 patients in the distal radial artery group (0.91% vs 0.31%, p=0.29).
- There were no differences in bleeding between groups, but the median time to hemostasis was shorter in the distal radial artery group compared to the traditional radial artery group (153 minutes vs 180 minutes, p=<0.0001).
The low rate of radial artery occlusion observed in the DISCO RADIAL trial is encouraging however the trial did not include patients with CKD.

A recent retrospective study by Yokota et al analyzed 117 patients receiving dialysis who underwent coronary angiography or PCI with distal radial artery access. In this study, cardiac catheterization using distal radial artery access was successful in 106 patients (90.5%). Proximal radial artery occlusion occurred in 3 out of the 85 patients (3.5%) and distal occlusion occurred in 5 out 85 patients (5.9%).

In summary, radial artery access offers significant benefits for coronary angiography and PCI when compared to the femoral artery access due to lower risk of bleeding and improved patient comfort. Several single-center studies have shown a lower rate of radial artery occlusion with the distal radial artery approach compared to the traditional radial artery approach. The recently published DISCO RADIAL trial demonstrated a low rate of radial artery occlusion with both radial artery approaches, highlighting that operator expertise, adequate anticoagulation and anti-spasmolytic therapy, use of slender sheaths and shorter hemostasis time can significantly lower the rate of radial artery occlusion regardless of the site of radial artery puncture. Robust data on radial artery access for cardiac catheterization in patients with CKD is lacking. Data from retrospective and observational studies shows a radial artery occlusion rate of 6.5% – 9.0% in patients with CKD who underwent cardiac catheterization via radial artery access. In patients with CKD, radial artery preservation for future AVF creation is preferred but lowering risk of periprocedural bleeding and improving patient comfort are also critical. Therefore, the decision to proceed with radial artery versus femoral artery access for coronary procedures in patients with CKD must be based on operator expertise, patient comorbidities, risk of bleeding, life expectancy, suitability of veins in the forearm/wrist for future AVF creation and patient preference. If radial artery access for a coronary procedure is selected in patients with CKD, then the distal radial artery is preferred to traditional radial artery access due to lower risk of proximal artery occlusion. Finally, in patients with CKD, an informed decision regarding arterial site of access for coronary procedures must be made on a case-by-case basis.
Reviewed by: Brian Rifkin, Margaret DeOliveira, Matthew A. Sparks
