
Maria Angela Matabang, MD
PGY-2 Medical Resident
Lincoln Medical Center
Ramani Karthik, MD, MHA, FACP, FASN, FASDIN
Medical Director of Interventional Nephrology
University of Michigan, FASDIN
Acknowledgements: This post is part of a collaboration between The Renal Fellow Network and the American Society of Diagnostic and Interventional Nephrology (ASDIN), whose mission is to provide excellence in dialysis access care to improve outcomes for patients with kidney disease. For more information about the ASDIN mission or membership, click here. Special thanks to the ASDIN Fellows Education Committee for their support on this project.
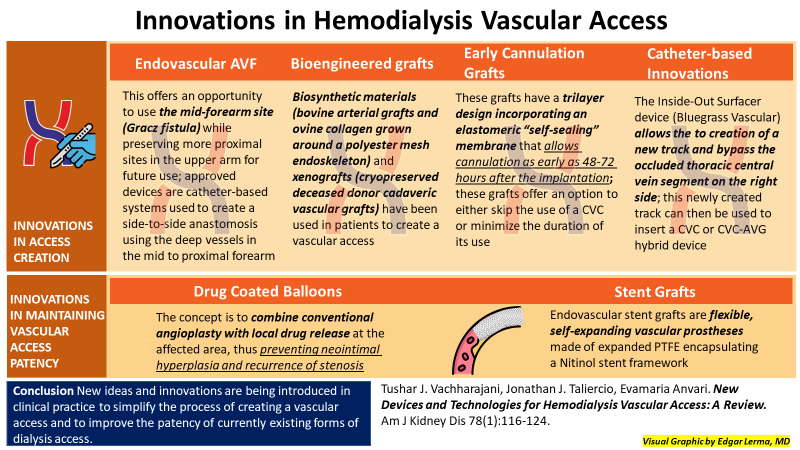
Chronic kidney disease (CKD) is present in an estimated 37 million US adults, and every 24 hours there are approximately 360 people started on dialysis for end stage kidney disease (ESKD). A diagnosis of CKD significantly impacts a patient’s quality and length of life. In addition, ESKD creates significant psychological and financial stress on patients and families. In fact, ESKD impacts the entire US economy, accounting for more than 50 billion dollars in US healthcare expenditure in 2020. Dialysis access creation, and subsequent dysfunction, is one of the causes for increased morbidity, mortality, and expense for patients on dialysis. In addition, female sex, advanced age and multiple comorbidities including diabetes mellitus, cardiovascular disease, obesity, and frailty are risk factors for a dysfunctional dialysis access. Recent efforts have emphasized improving, and further innovating upon, dialysis access creation and preservation of access patency.
Endovascular AVF Creation
Novel and less invasive surgical techniques are being used to create arterio-venous fistulas (AVFs) for dialysis. Endovascular AVFs (endoAVF) are created percutaneously with one or two vessel cannulations and specialized catheters that create an arterial-venous anastomosis with either magnets or heat and pressure. The eligibility factors for an ideal recipient of an endoAVF include life expectancy of at least 1 year, vessels that are unsuitable to surgically create a distal AVF, a compressible proximal radial/ulnar artery without intimal calcification, an inflow brachial artery ≥2 mm, an outflow cephalic and/or basilic vein ≥2.5 mm, procedural access vessels >2 mm, a perforator ≥2 mm and not tortuous, and an adequate creation site with ulnar and/or radial target vessels >2 mm. Since endoAVF creation can be done in an office setting (versus a hospital based operating room), delays in AVF creation due to scheduling can be improved. Another advantage of endoAVFs is that flow dynamics are thought to be better at reducing shear stress and neointimal hyperplasia, compared with surgical AVFs, reducing the risk of stenosis. Lastly, endoAVF creation reduces local inflammation with the avoidance of surgical dissection, minimizes vessel wall trauma, and eliminates the need for sutures. EndoAVFs (Figure 1) still need long-term randomized controlled studies and more widespread trained experts before they become a more popular option. High success rates in early studies, in the hands of experienced operators, seem promising in selected patients.
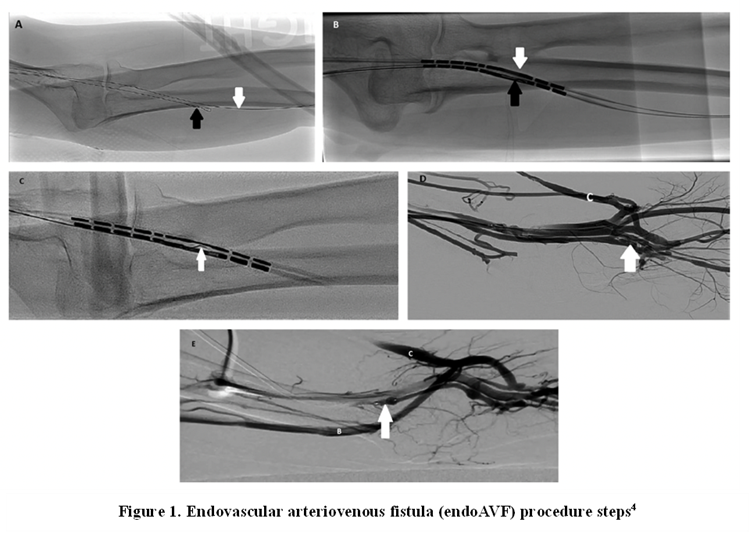
Figure 1. EndoAVF creation. Ulnar artery (white arrow), ulnar vein (black arrow)
Drug-Coated Balloons
Neointimal hyperplasia of a fistula or graft, followed by stenosis of the dialysis access with reduced blood flow, is a frequent complication of dialysis access. Dialysis access patency requires vigilant screening and often repeat interventions. Percutaneous catheter-based angiograms with balloon angioplasties are a common procedure in interventional nephrology practices. New innovations to maintain patency include the use of drug-coated balloons (DCB) (Figure 2). Endothelial injury secondary to the forceful vessel dilatation from balloon angioplasty may create deep tissue damage, creating a recurring cycle of inflammation and neointimal hyperplasia vessel stenosis. Paclitaxel is a cytotoxic agent which stops the M-phase of mitosis and halts neointimal hyperplasia via cellular apoptosis and inhibition of migration of vascular smooth muscle into the intima. In 2017, the FDA approved the first DCB to treat stenosis in a dialysis vascular access. The method of drug delivery is critical, as very slow or very fast delivery could result in subtherapeutic levels, and intervention failure. The use of a DCB is a promising therapy, but long-term efficacy and safety data collection is still ongoing. The role of DCB to treat access stenosis remains controversial as one recent meta-analysis of 17 studies showed better primary patency at one year and one meta-analysis of 11 studies did not show improved patency. The cost of DCBs also limits their use in office based or ambulatory surgical centers.
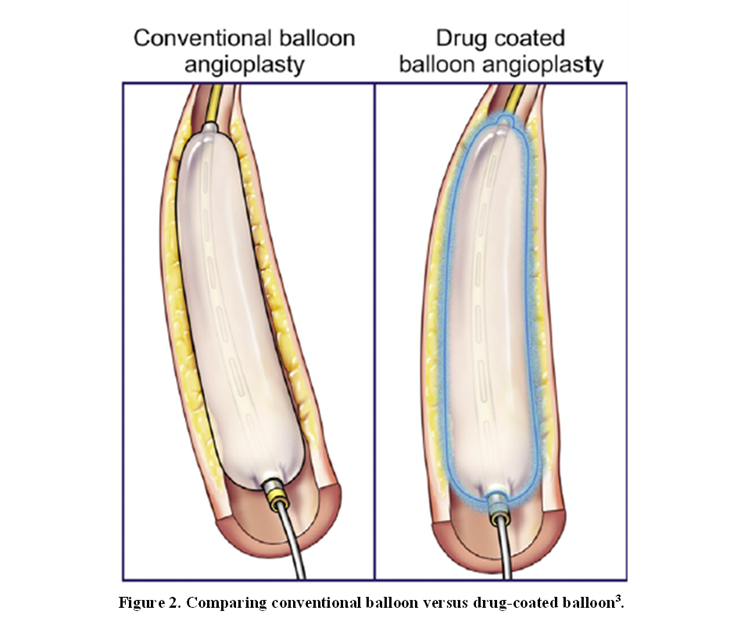
Figure 2. Drug coated balloon angioplasty
Tissue-Engineered Vascular Grafts
A mature AVF is still the gold standard for long-term maintenance hemodialysis. The dogma has shifted from “fistula first” to “the right access, at the right time, in the right patient”. Over the last 2 decades, after gathering clinical evidence, alternative types of access were given equal importance with emphasis on implementing a patient-centered approach. KDOQI now advocates for establishing an ESKD life-plan for dialysis access choice.
An arterio-venous graft (AVG) is a piece of polytetrafluoroethylene (PTFE) plastic that is interposed between a vein and an artery to create a dialysis access circuit. The indication for an AVG can be exhaustion of superficial venous beds or unsuitable, small vessels. It may also be secondarily indicated following a failed previous AVF. AVGs have a lower primary 1-year patency at 51% compared with AVFs at 86%. Moreover, AVGs are accompanied by various complications including frequent thrombosis, poor durability, material degradation and infection. To address these complications nearly three-quarters of a century has been spent to develop bioengineered tissue grafts. The ultimate purpose of these tissue-engineered vascular grafts (TEVG) is to create an access that can maintain patency, endure regular needle cannulation, and resist infection.
TEVGs are categorized into 3 groups: grafts created in vivo by “bioreactors”, scaffold-based TEVGs and sheet-based TEVGs. Grafts created in vivo by “bioreactors” are prepared by implantation of a foreign body or cylindrical mandrel into a host. This results in a foreign body reaction, and formation of connective tissue that can be used as a vascular conduit. Omniflow is a glutaraldehyde-tanned ovine collagen tube grown around a Dacron mesh template in a sheep bioreactor. A newer version, Omniflow II showed much improved primary and secondary patencies, approaching that of AVF.
Next, the prototype of scaffold-based TEVGs used bovine aortic tissue. The process took around 4 to 6 weeks, at which point a rigid scaffold was created in vitro. However, the products created were either too weak to support high pressure, or prone to degradation and did not match the compliance of autologous vessels. Eventually, biodegradable and xenogeneic tissue scaffolds were developed and decellularized vessels were made. Decellularization is the most effective process of removing antigenic material from both native or bioengineered vessels.
In 2004, the first phase I/II clinical trials using autologous cells to create a patient-specific bioengineered vessel for re-implantation as a dialysis access. A sheet-based technology was utilized, which was made by growing the recipient’s own fibroblast cells taken from biopsy. The resulting sheet of cellular material was then wrapped around a mandrel multiple times, allowed to incubate and then seeded with the recipient’s autologous endothelial cells prior to implantation.
In another attempt to create a TEVG, phase II clinical trial using human acellular vessels (HAV) as a conduit for HD access in 2012. This was produced by getting smooth muscle cells harvested from deceased human organs and tissue donors. These were then grown in a nutrient medium and seeded into a biological scaffold placed in a bioreactor. A pulsatile flow of nutrient-rich fluid was provided by the bioreactor, exposing cells to shear stress and eventually promoting cell differentiation.The graft was then decellularized to remove antigens, leaving the nonimmunogenic collagen tube behind (Figure 3).
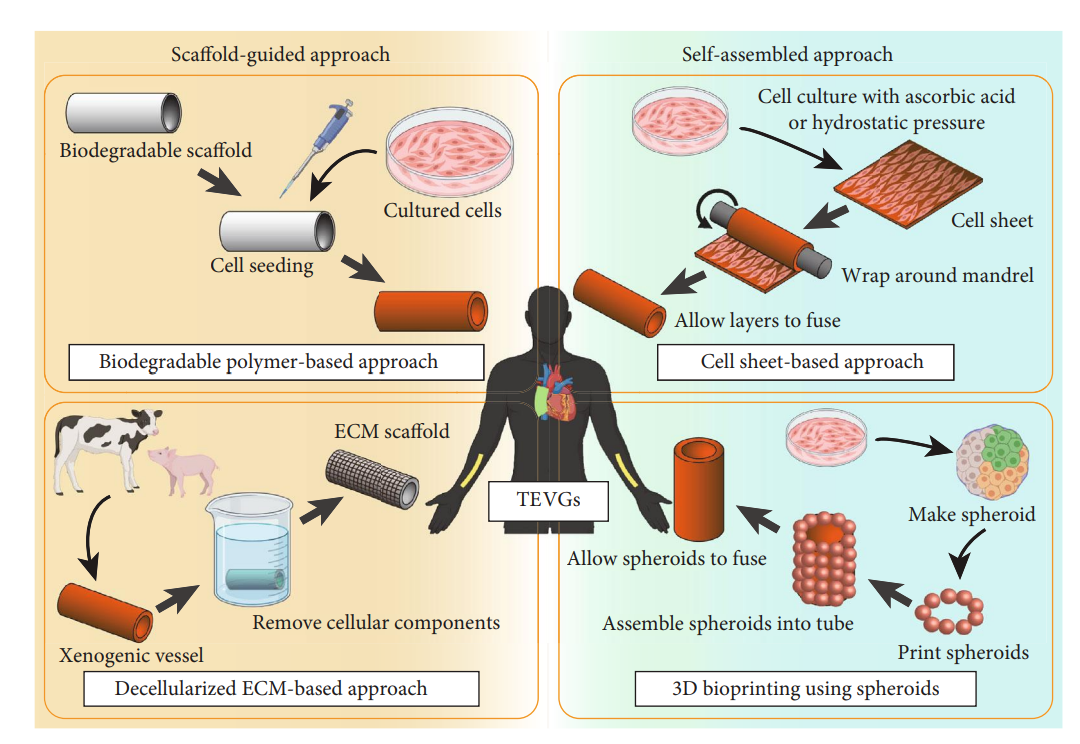
Figure 3. Bioengineered vessel mechanisms
The phase 2 trial results for HAV grafts were published in 2016. It included a total of 60 patients (20 from the United States and 40 from Poland), who were followed for 16 months. Results showed that the primary patency (intervention-free access survival) rates were 63% and 28%, at 6 and 12 months respectively. Primary assisted patency (durability of an intervention until the first episode of thrombosis) rates were 73% and 38% respectively. Secondary patency (durability of intervention until the access is abandoned) rates were 97% and 89%, respectively. Moreover, the study also confirmed the absence of a systemic immune or inflammatory response. Another fascinating outcome was the identification of CD68 and CD31 cells as early as 16 weeks on segments of HAV graft near the venous anastomosis site and previous cannulation sites. The presence of these cells indicated the surrounding connective tissue cells repopulated the HAV graft. This suggested creation of a “living tissue” which was capable of self-healing after cannulation. Given the success of the early trial, there is now enrollment of a multicenter, randomized, controlled phase 3 trial comparing HAVs to AVFs. It includes 240 HD patients and is expected to be completed in June 2024.
The future is exciting, and the portfolio of options available for patients with end stage kidney disease is undergoing a paradigm shift. A patient centric personalized approach for access creation and maintenance will help physicians and patients align their shared goals. With many more innovations in the pipeline, dialysis access transformation will continue to strive to make dialysis less burdensome for patients and caregivers. These innovations have the potential to reduce patient discomfort that can be associated with dialysis access creation and maintenance. Ultimately, technological advances may assist in creating a single, durable, regenerative access that will last the entire duration of dialysis therapy with minimal need for interventions and negligible risk of infection and thrombosis.
Reviewed by: Brian Rifkin , Edgar Lerma, Sam Kant, Margaret DeOliveira