Welcome to the 35th case of the Skeleton Key Group, a team of nephrologists from around the world who build a periodic education package for the Renal Fellow Network.
Authors: Marc Soco (@msocoMD)
A. The Stem
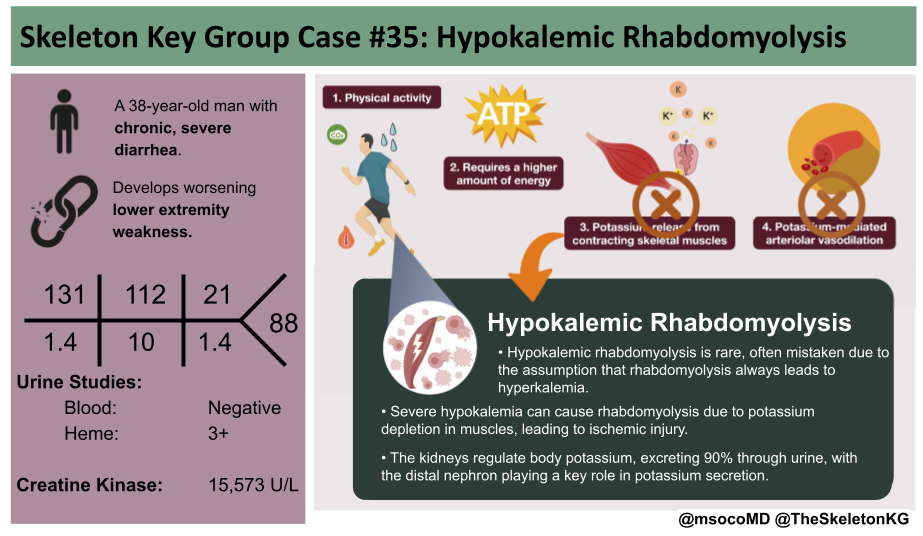
A 38-year-old man presents to the emergency department with bilateral lower extremity weakness. For the last three months, he reported fatigue, anorexia, and weight loss. Two months ago, he developed loose-to-watery stools, up to five times-a-day. He has been self-medicating with loperamide, without relief. Three days before admission, he noted muscle weakness primarily in the legs and on the day of admission he was unable to get out of bed.
Past medical history indicated no prior conditions or hospitalizations. There was no relevant social, drug, or sexual history.
Vital signs:
BP 90/60 mm Hg
HR 91 bpm
RR 18 breaths per a minute
T 98°F
Oxygen saturation 97%
Physical examination:
General: not in any apparent distress
Neck: no jugular venous distention
Heart: no murmurs
Lungs: clear to auscultation bilaterally, not in respiratory distress
Abdomen: soft, non-tender, non-distended
Skin: normal skin turgor
Extremities: no lower extremity edema
Neurological: hypotonia and decreased muscle strength (1/5) in both legs with diminished deep tendon reflexes
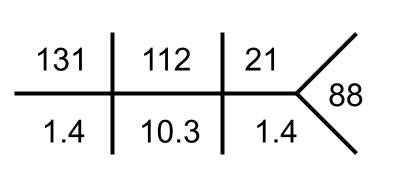
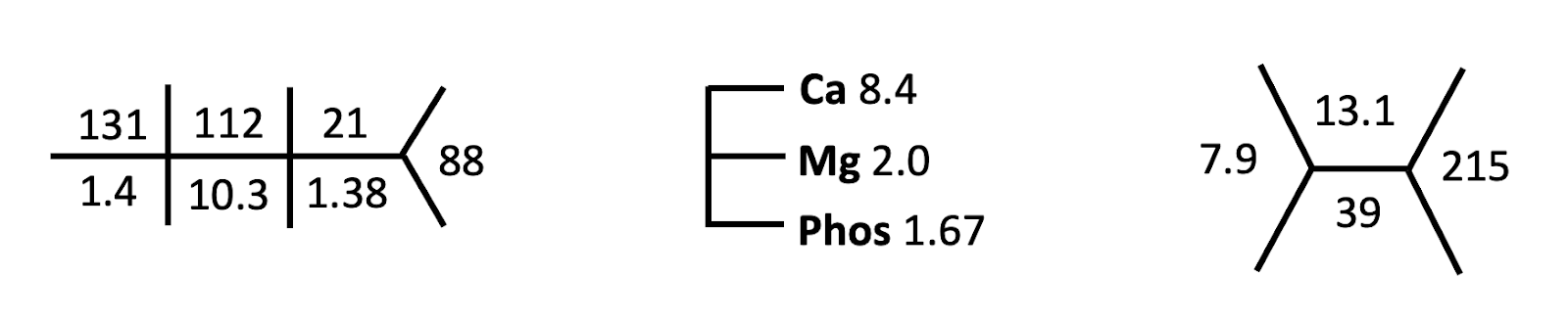
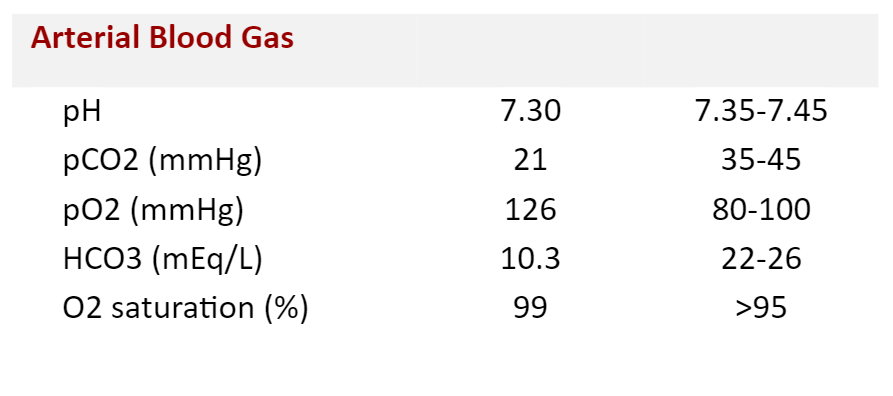
B. The Labs

C. The Workup
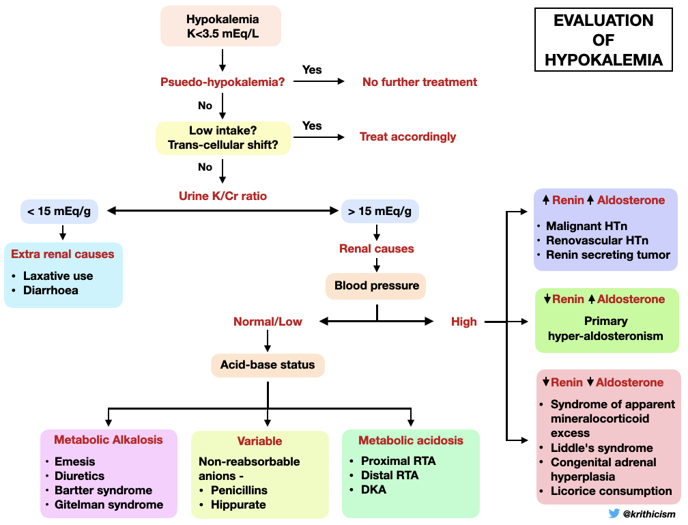
A man with persistent diarrhea and significant weakness presented with hypokalemia. The cause is likely diarrhea. However, let us go over this algorithm to review our systematic approach to hypokalemia as a review.
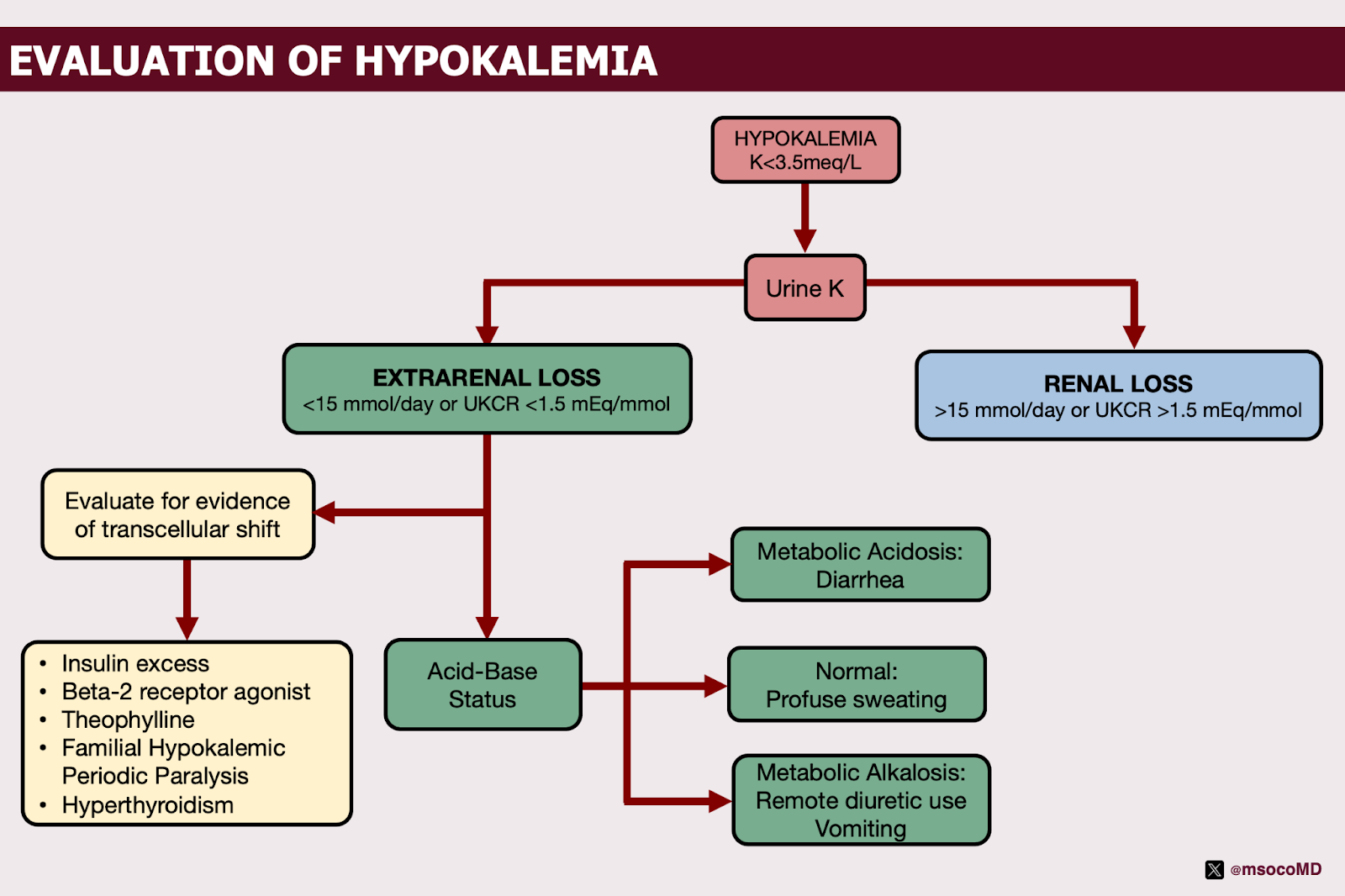
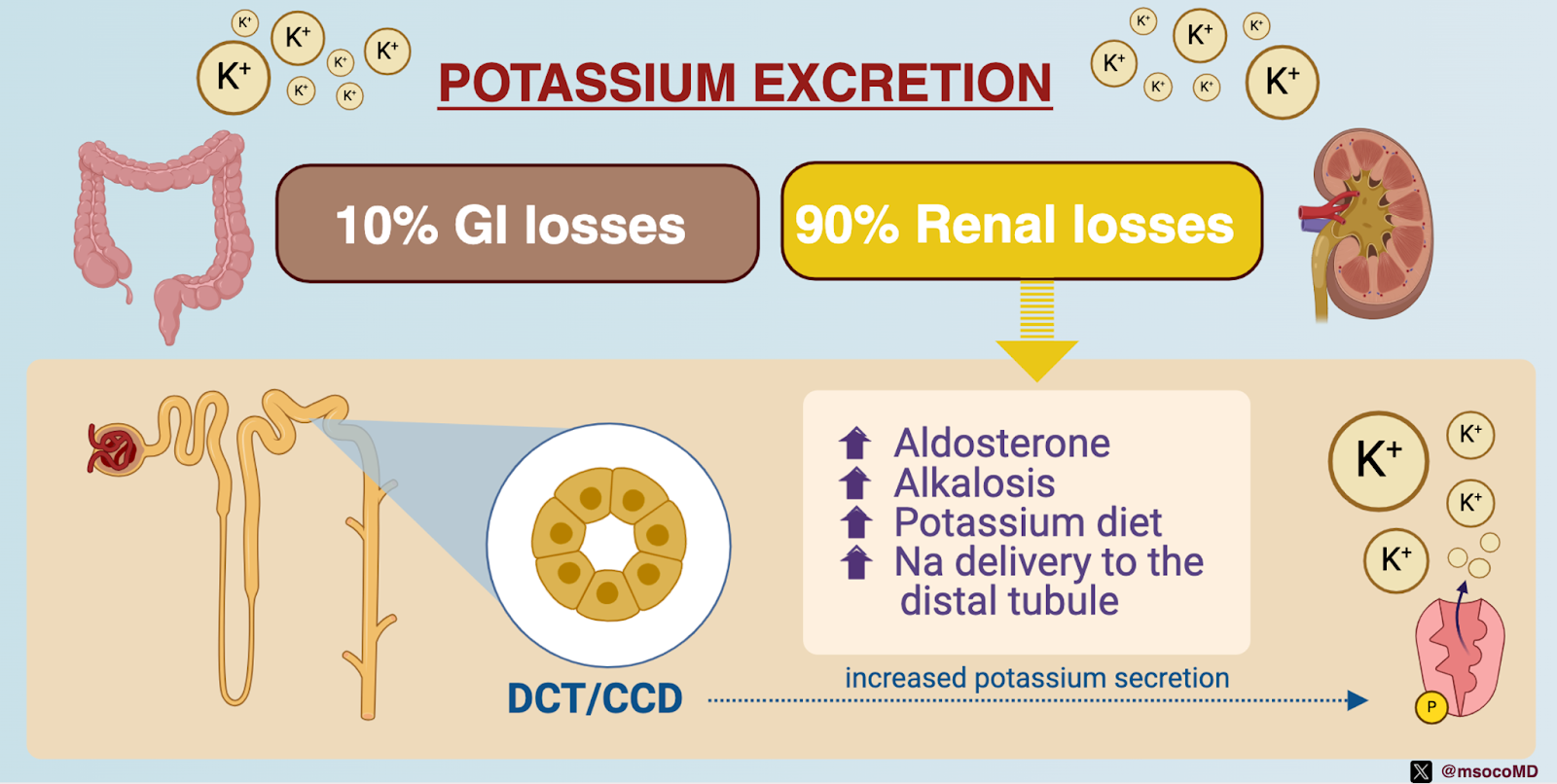
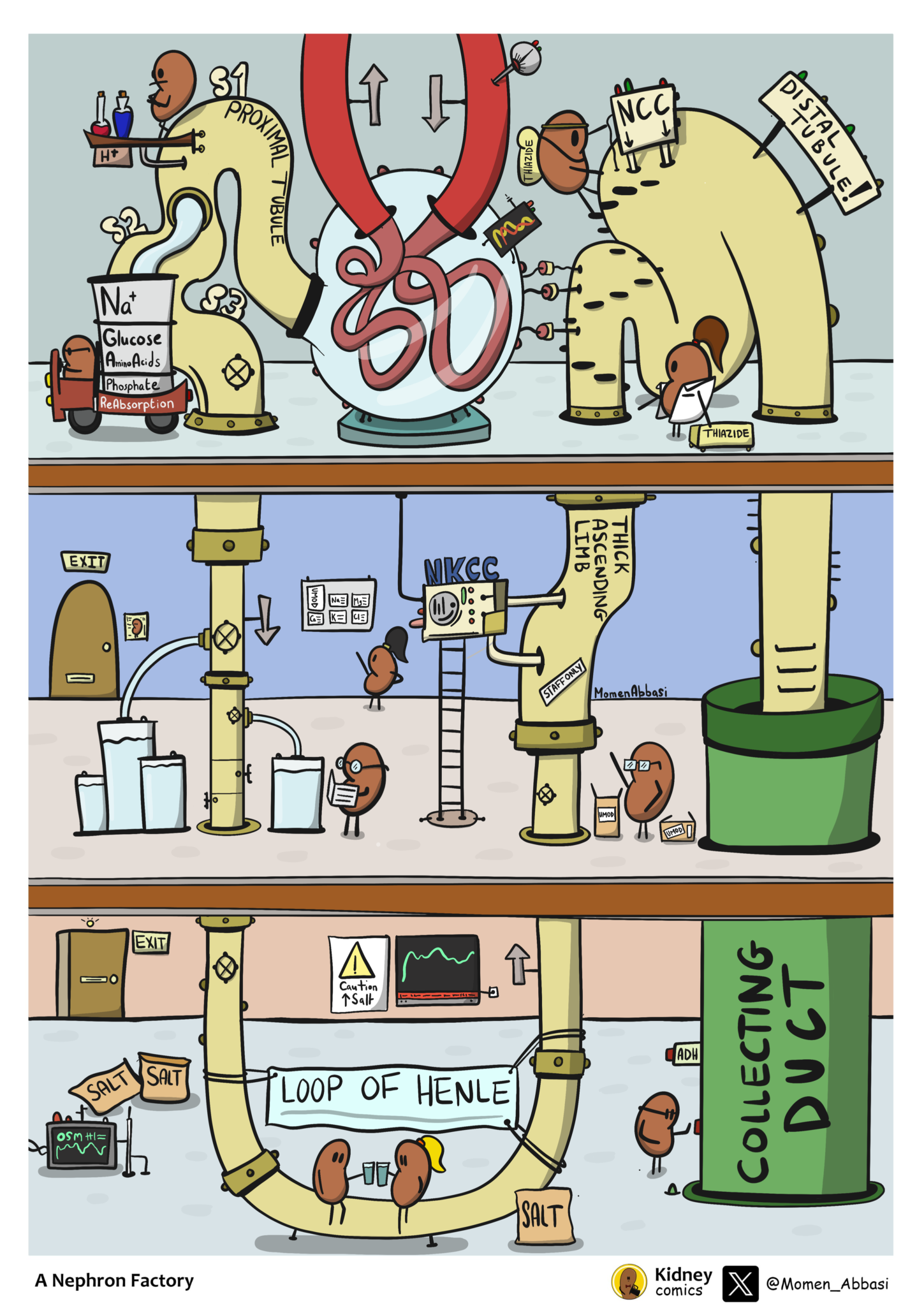
In the absence of evidence of a transcellular potassium shift– such as insulin excess, use of beta-2 agonists, theophylline, thyrotoxicosis, and familial hypokalemic periodic paralysis, urine potassium can be helpful to determine the etiology of hypokalemia. Kidney regulation of potassium excretion is pivotal to maintaining potassium balance. Individuals typically consume 60 to 100 mEq of potassium daily and essentially all of it is absorbed. Only about 10% of this potassium is lost through stool. Leaving 90% of dietary potassium to be excreted by the kidneys. The kidneys regulate total body potassium primarily through the activity of the distal nephron (check out SKG Case #31 for a detailed look at tubular handling of potassium). Potassium excretion is enhanced by aldosterone, alkalosis, adaptation to a high potassium diet, and increased sodium and tubular fluid delivery to the distal tubule.
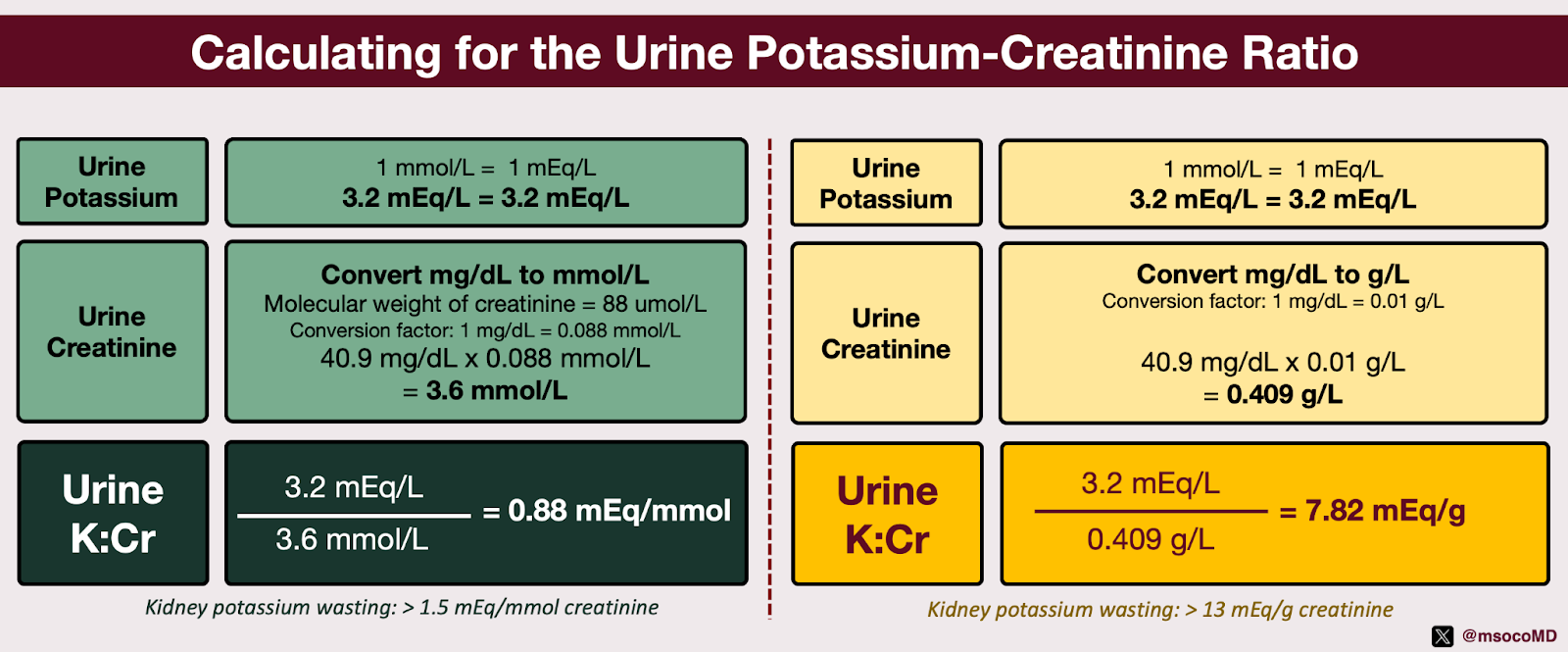
Evaluating renal potassium wasting is best accomplished by measuring potassium excretion in a 24-hour urine collection. However, this is difficult and time consuming. We use the urine potassium-to-creatinine ratio derived from a spot collection. Notably, values higher than 13 mEq/g creatinine (equivalent to 1.5 mEq/mmol creatinine) correlate with kidney potassium wasting. Upon investigation, the urinary potassium and urinary creatinine levels were measured at 3.2 mEql/L and 40.9 mg/dL, respectively.
Based on these values, we calculated the urinary potassium-creatinine ratio to be 0.88 mEq/mmol (7.82 mEq/g), indicating an extrarenal loss of potassium.
Having ruled out other potential causes, such as transcellular shifts, remote diuretic use, and profuse sweating, ABG and urine electrolytes were utilized to confirm that diarrhea was indeed the cause.
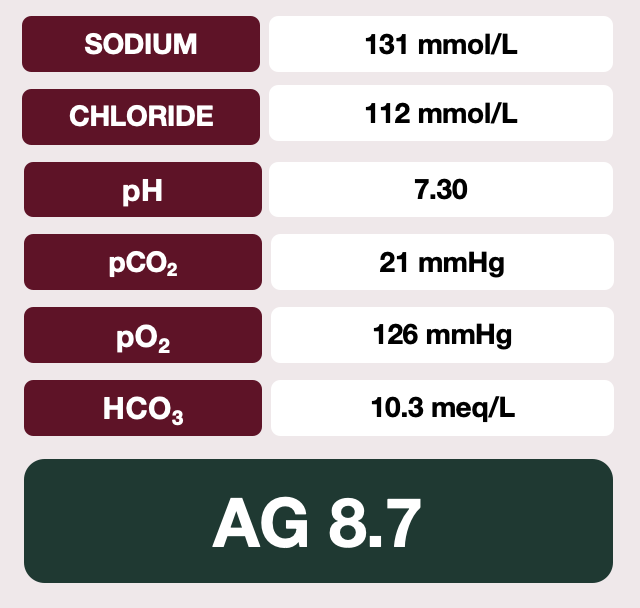
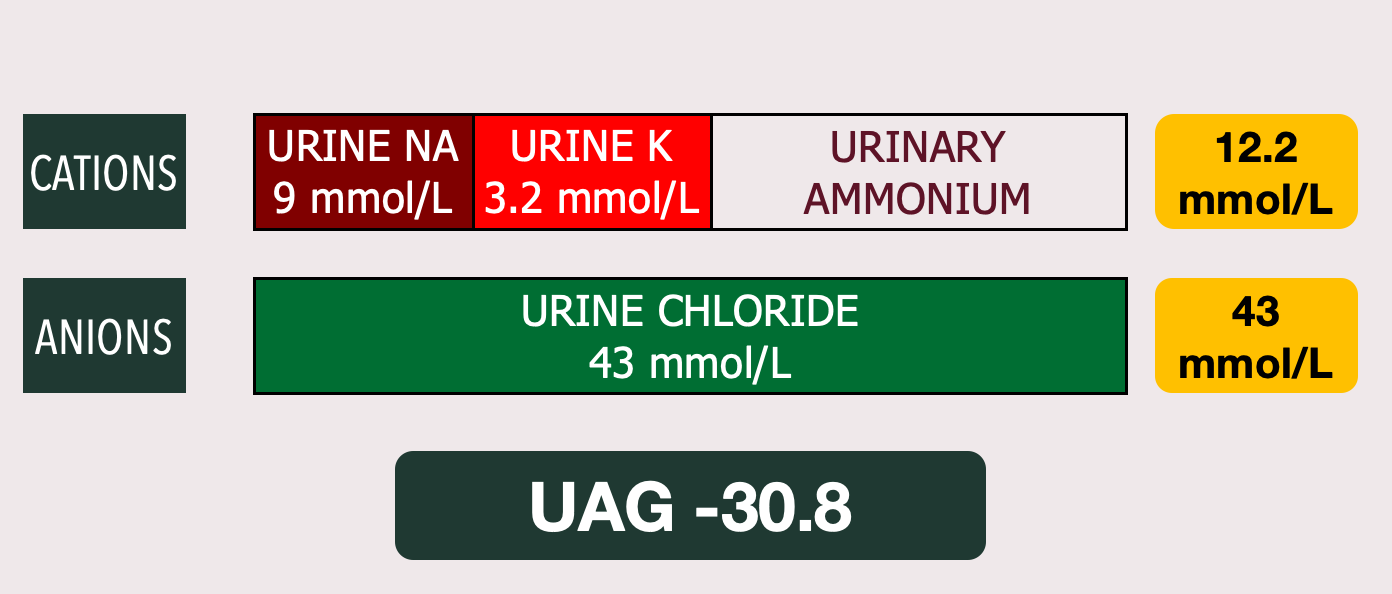
Physiologically, large volume or chronic diarrhea results in the parallel loss of sodium, potassium, bicarbonate, butyrate, citrate, and lactate in the stool, leading to a non-gap metabolic acidosis. The acidosis prompts increased renal ammonium (NH4+) synthesis and excretion. While clinical laboratories don’t typically measure urinary NH4+ excretion, it can be measured indirectly by calculating the urine anion gap (UAG = [Urine Na + Urine K] − [Urine Cl]). The presence of NH4+ is indicated when the sum of major cations (Na+, K+) is lower than the concentration of Cl− in the urine. A negative urine anion gap (more than –20 mEq/L) suggests the presence of appropriate urinary NH4+ with the acidosis, as may be observed in cases of diarrhea. As shown above, our calculations have shown a normal-gap metabolic acidosis and a negative urine anion gap, consistent with gastrointestinal losses as the root cause.
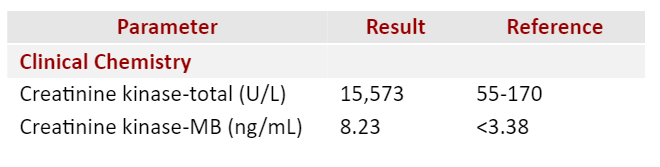
Moving forward, it’s worth noting that the urinalysis interestingly showed the presence of heme, even though no red blood cells were found (indicative of myoglobinuria). Rhabdomyolysis was later confirmed when we found myoglobin in the urine and a significantly high level of serum creatine kinase (15,573 U/L).
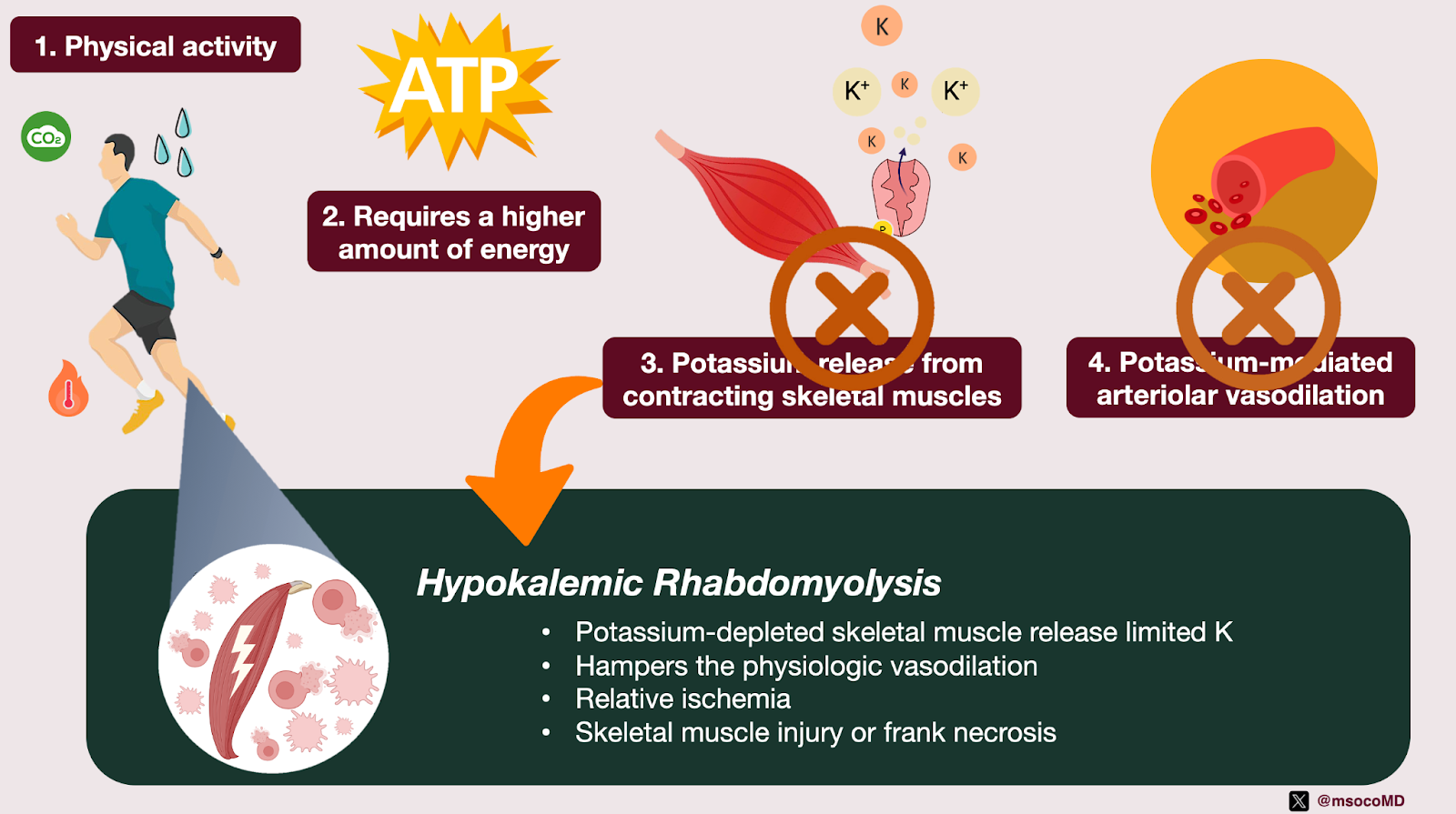
The rare association of rhabdomyolysis with hypokalemia represents an interesting display of physiology. When we engage in physical activity, our skeletal muscles require increased blood flow. This hyperemic response is partially facilitated by the release of potassium from contracting skeletal muscles causing arteriolar vasodilation and improving regional blood flow. However, in severe hypokalemia, potassium-depleted skeletal muscles release limited potassium, hampering this physiologic vasodilation, which may lead to skeletal muscle ischemia.
As previously discussed, only 10% of the daily potassium intake is lost in the stool. In order for hypokalemia to be severe enough to induce rhabdomyolysis, diarrhea must be excessively voluminous or chronic. Further investigation of the chronic diarrhea showed a cryptosporidium stool antigen. After obtaining consent, a Human Immunodeficiency Virus (HIV) test was conducted and was positive. Colonoscopy showed chronic active colitis with erosions, cryptitis, and hemorrhage.
D. The Diagnosis and Management
This was a 38-year-old man with 2 months of diarrhea who presented with symptomatic hypokalemia. Subsequent workup revealed a urine potassium-creatinine ratio of 0.88 mEq/mmol (7.82 mEq/g), normal anion gap metabolic acidosis, negative urine anion gap, and an elevated serum creatine kinase, consistent with a diagnosis of hypokalemic rhabdomyolysis from chronic diarrhea. Further investigation disclosed a diagnosis of cryptosporidiosis as the underlying cause of the diarrhea.
Isotonic saline was given to ensure adequate urine output. Additionally, intravenous and oral potassium supplementation was given to replenish the potassium. Cryptosporidiosis was managed symptomatically with the primary focus of restoring immune function. He had follow-up with an ID specialist. Upon follow-up, no additional complaints surfaced, nor were there any signs of recurring diarrhea. Furthermore, laboratory tests indicated that the serum electrolytes were in the normal range.

E. Take Home Points
- Hypokalemic rhabdomyolysis is unusual and may be underrecognized given that rhabdomyolysis typically leads to hyperkalemia due to cellular breakdown and subsequent kidney failure.
- The body excretes about 90% of its daily potassium through urine and the remaining 10% through stool. The kidneys regulate total body potassium, with the distal nephron’s potassium secretion into urine being a key component.
- Large volume or chronic diarrhea can cause normal-anion gap metabolic acidosis due to the loss of sodium, potassium, bicarbonate, butyrate, citrate, and lactate in the stool.
- In diarrhea, there is a parallel decrease in urinary excretion of sodium and potassium, while urinary chloride excretion remains relatively constant. Ammonium and chloride are the primary electrolytes excreted in the urine, resulting in a negative urine anion gap.
- Severe hypokalemia can cause rhabdomyolysis because potassium-depleted skeletal muscles release limited potassium, hindering physiologic vasodilation. This may lead to skeletal muscle injury or necrosis due to relative ischemia.
Editors: Jefferson L Triozzi, Chi Chu, Sacha Moore, Joel Topf, Margaret A. DeOliveira, Matthew A. Sparks

{kind=link}