Welcome to the 37th case of the Skeleton Key Group, a team of nephrologists from around the world who build a periodic education package for the Renal Fellow Network.
Author: Carolina Mendez ( @carolinaanalis1) and Ana Hernandez ( @AnaHernandezMD)
A. The Stem
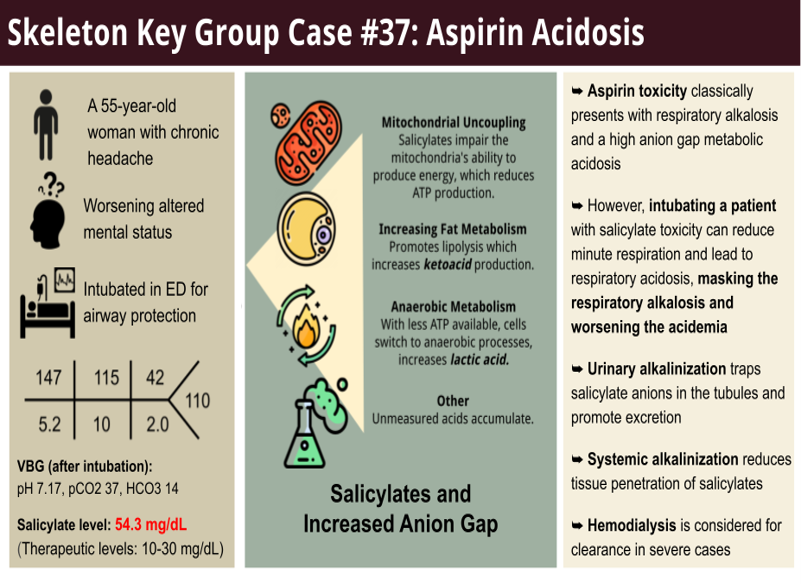
A 55-year-old woman with a history of Roux-en-Y gastric bypass, anxiety, depression, and chronic migraines was brought in by her family due to altered mental status. The patient had reported a worsening of her migraines over the past few days and increased her dosage of aspirin. She was also found to be confused for several days, reported difficulty upon awakening, and increased respiratory effort. On presentation to the emergency room, she was intubated in triage for airway protection, given her severely altered mental status.
Vital signs after intubation:
T 37.3 celsius
HR 97 bpm
RR 21 per minute
BP 109/61 mm Hg
SpO2 98%
Physical Exam:
Gen: ill appearing and intubated
Heart: accelerated HR, regular rhythm
Lungs: soft bilateral breath sounds
Abdomen: soft and nontender
Extremities: no lower extremity edema, no skin changes
Neurological: sedated (Glasgow Coma Scale 3)
B. The Labs
Imaging:
No significant findings. Normal head CT.
C. The Workup
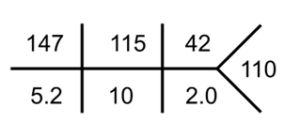
Our patient’s VBG on presentation:
How to determine the primary acid/base disturbance
Table1 Key : ↓ ↑ = compensatory response
Let’s break it down!
1. First, assess the pH
- A normal pH is 7.35-7.45
- A pH < 7.35 represents acidemia
- A pH > 7.45 represents alkalemia
This patient has a VBG pH of 7.17, acidemic
2. Next, look at labs: HCO3 and pCO2.
This patient has a primary metabolic acidosis because the HCO3 was 10 (low), and pCO2 was 37 (normal).
3. Now calculate the anion gap (AG)
- AG = Na – ( Cl + HCO3)
- To confirm an elevated AG, use the patients’ albumin (an anion) to find their expected anion gap.
- Expected AG: albumin x 2.5
This patient has an anion gap of 22 (Na 147 – (Cl 115 + HcO3 10 = 22), her expected anion gap based on albumin of 4 x 2.5 is 10. This confirms a high anion gap metabolic acidosis (HAGMA). Use the GOLDMARK to remember the potential causes of an anion gap:

Figure 1: Causes of anion gap metabolic acidosis NephSim
4. Now check for appropriate compensation
- Now, we can determine if the body has compensated or if other acid-base disturbance(s) are present. Respiratory compensation happens relatively quickly, while metabolic (kidney) may take a few days.
- Use Winters’ formula to determine how pCO2 should compensate for a metabolic acidosis: expected pCO2 = 1.5(HCO3) + 8
Using Winter’s formula, this patient has an expected pCO2 due to compensation of 23 (pCO2 = 1.5 (10) + 8 = 23) but the patient’s measured pCO2 is 37; this indicates a concomitant respiratory acidosis.
5. Calculate the Delta Delta Ratio (Δ/Δ)
- Calculate the Delta Delta Ratio in patients with a HAGMA to determine if a mixed acid-base disorder is present.
- Δ/Δ = (anion gap – normal anion gap) / (normal HCO3 – HCO3)
- The Delta Delta ratio compares the rise in the anion gap to the fall in HCO3.
- This ratio should be between 1-2 if only an uncomplicated anion gap metabolic acidosis is present
This patient has Δ/Δ = (22-10) / (24-10) = 0.85; which confirms an additional normal anion gap metabolic acidosis.
In summary, the patient displayed a mixed acid-base disorder:
-Anion-gap metabolic acidosis
-A normal anion gap metabolic acidosis
-A respiratory acidosis
In solving acid-base problem you can use pLACO
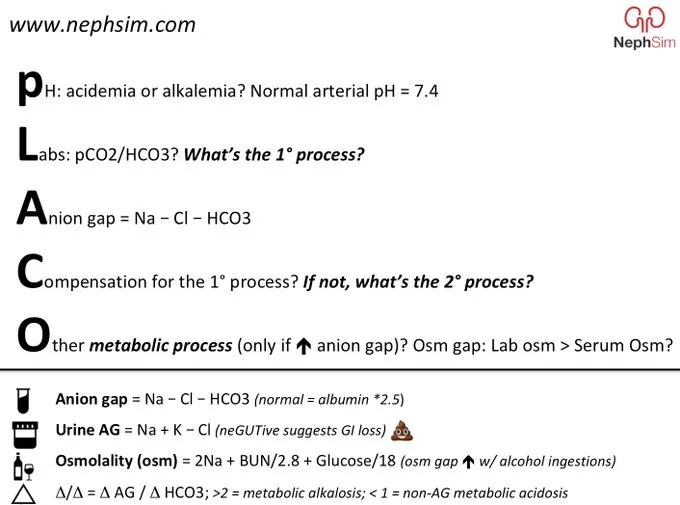
Figure 2: Nephsim trick to solving every acid/base problem: pLACO
D. The Diagnosis
This was a 53-year-old woman who presented with migraine, altered mental status, and increasing respiratory difficulty. The patient’s medication list was notable for aspirin. The patient’s daughter reported an increase in the patient’s aspirin dosage, given the progressive nature of her recent migraines. The workup showed a mixed acid-base disorder. Subsequent toxicology screening demonstrated elevated salicylate levels suggestive of aspirin toxicity
Patient’s Toxicology Report
But wait a minute… didn’t we learn that aspirin toxicity classically presents with anion-gap metabolic acidosis and respiratory alkalosis? This patient deviates from the traditional teaching. Let’s explore why.
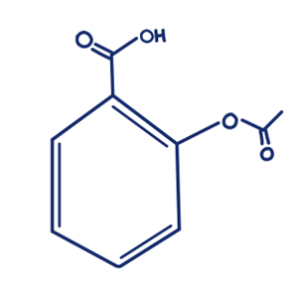
Figure 3: Salicylate molecule: Image: Carolina Mendez
Aspirin toxicity:
Aspirin (acetylsalicylic acid) is easily absorbed in acidic environments like the stomach due to its ionization constant pKa of 3. Therapeutic salicylate levels typically range from 10-30 mg/dL, levels above 40-50 mg/dL are toxic, and concentrations exceeding 70 mg/dL are considered seriously toxic. Several factors influence the severity of toxicity, including co-ingestion of other substances, delayed gastric emptying or slow transit of aspirin formulations, and the type of aspirin formulation consumed.
- Therapeutic levels: 10-30 mg/dL
- Toxic levels: 40-50 mg/dL
- Seriously toxic levels : >70 mg/dL
Acid-Base Disorders in Salicylate Toxicity: Classically a respiratory alkalosis and high anion gap metabolic acidosis
In most salicylate toxicity cases, the earliest acid-base disturbance is respiratory alkalosis, occurring in approximately 20% of cases. Salicylates stimulate the respiratory center in the medulla, resulting in hyperventilation. Increased respiratory rate and hyperpnea can cause excessive elimination of carbon dioxide and an increase in blood pH (alkalemia). As aspirin toxicity progresses, high anion gap metabolic acidosis typically develops due in part to salicylic acid derivatives but also the development of lactic acid/ketoacids. As salicylate is metabolized predominantly in the liver, it causes the uncoupling of oxidative phosphorylation and impairs ATP production. The increase in anaerobic metabolism leads to lactic and keto acid buildup. Interestingly, the acidemia facilitates salicylates’ ability to cross the blood-brain barrier, further stimulating the respiratory center. It creates a feedback loop of hyperventilation and worsening respiratory alkalosis.
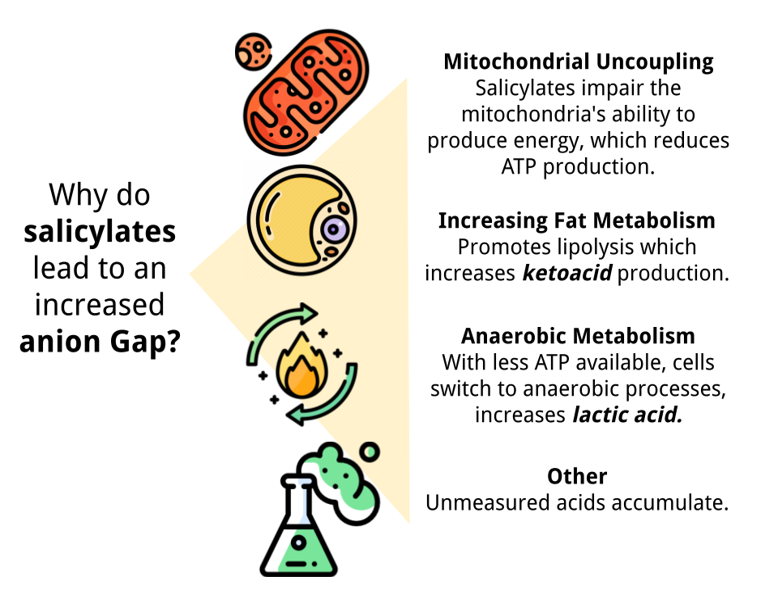
Figure 4: Etiology of increased anion gap in salicylate toxicity. Original image derived from explanations and figures from Palmer et al.
So, what is going on with our patient?
Our patient demonstrates an anion gap metabolic acidosis due to salicylate derivatives. On admission, lactic acid was measured to be 1.6 mmol/L and within normal limits. However, our patient has respiratory acidosis, not a respiratory alkalosis as usually described. Remember that salicylate crosses the blood-brain barrier and stimulates the medullary center to increase respiration, leading to respiratory alkalosis. However, intubating a patient with aspirin toxicity introduces several challenges in patients with salicylate toxicity. Intubation and sedation blunt the patient’s hyperventilatory drive. Without compensation, the pre-existing respiratory alkalosis may rapidly transition to respiratory acidosis. Furthermore, the acidotic state promotes the protonation of salicylate anions (charged) into uncharged salicylic acid (uncharged), increasing intracellular drug penetration into the brain. In this case, intubation and sedation were necessary for airway protection (life-saving ABCs: Airway Breathing and Circulation). However, precaution must be taken when intubating a severely acidotic patient. In preparation for intubation, consider fluid resuscitation utilizing D5 to treat CNS hypoglycemia and sodium bicarb to treat metabolic acidosis. Sedation for endotracheal intubation and mechanical ventilation may cause transient hypoventilation and associated respiratory acidosis. Avoid keeping salicylate-poisoned patients in conventional ventilator settings, as their spontaneous respiratory alkalosis will be abolished, and their clinical condition may deteriorate. It’s essential to prioritize increasing the respiratory rate to lower the PaCO2 and compensate for the acidosis.
Finally, we observed a concomitant normal anion gap metabolic acidosis. Roughly 20% of patients with aspirin toxicity can have NAGMA due to several mechanisms. NAGMA typically results from kidney bicarbonate losses (HCO3-) with sodium and potassium salts. As bicarbonate is excreted, serum chloride levels increase proportionally to maintain electroneutrality, resulting in a normal anion gap. However, in salicylate toxicity, the appearance of a NAGMA could also be due to laboratory error. This interference seems multifactorial in etiology- likely due to the loss of selectivity of the chloride electrode and competition between chloride and salicylate to bind albumin. If that were to happen in our case, this erases the NAGMA: to see how, convert the salicylate level of 54 mg/dl to mEq/L (by dividing by the molecular weight of salicylates of 137 and multiplying by 10) which equals 4 mEq/L. If you take the measured Cl of 111 and add 4 mEq/L, you get 115 and a new anion gap of 26. This results in a normal gap-gap, (26-10) / (24-1), of 1.14.
E. Management
For management, it’s important to restore fluid status in volume-depleted patients. Hyperventilation, fever, and alterations in metabolic activity contribute to hypovolemia. Patients should be admitted to the intensive care unit and reported to toxicology. Once the patient is stabilized, efforts should be made toward reducing salicylate levels. Studies have shown that aspirin is well absorbed by activated charcoal if in an acute overdose. The recommended dose is three 25-gram doses separated by two hours.
Gastrointestinal decontamination techniques such as whole bowel irrigation and activated charcoal administration may be considered in some cases. Patients presenting early after ingestion or with increasing absorption levels may be good candidates. Otherwise, gastrointestinal decontamination is a futile endeavor.
Urinary and systemic alkalinization can be done by administering 1-2 meq/kg of bicarbonate followed by bicarbonate drip. Urine alkalization is important as it traps the salicylate anion in the renal tubule. Systemic alkalization prevents diffusion of the non-ionized form back into tissue. The goal urine and serum pH is ≥7.5. During alkalinization therapy, calcium should be monitored closely due to the risk of hypocalcemia.
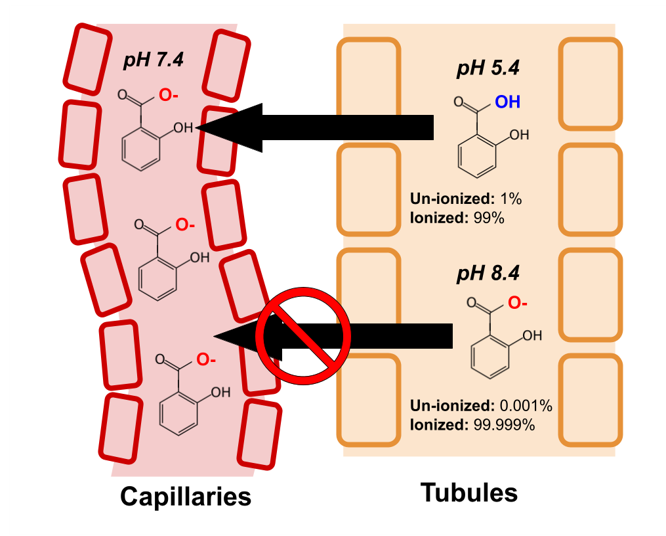
Figure 5: Urine alkalinization leads to decrease in un-ionized fraction in the tubular lumen. Original graphic derived from figures by Palmer et al.
Aspirin ionizes (loses an H) at higher pH. Aspirin does not cross the biological membranes when it is ionized. Most of aspirin is ionized in the blood. This is why urinary alkalinization enhances the elimination of aspirin.
Hemodialysis may be indicated if toxicity is severe based on symptoms or when salicylate levels are >100 mg/dl. For example, hemodialysis should be initiated even if salicylate levels are less than 100 mg/dl if the patients also have AKI, hyperthermia, non-cardiogenic pulmonary edema, or CNS involvement (for example, altered mental status, cerebral edema, or seizures, etc). While this patient’s salicylate level was less than 100 mg/dl, she did receive hemodialysis due to her altered mental status with acute kidney injury.
Table is from EXTRIP Workgroup. The EXTRIP (extracorporeal treatments in poisoning) is an excellent resource for guidance on the use of dialysis in toxicology settings (extrip-workgroup.org).
F. Take Home points
- Aspirin toxicity classically presents with respiratory alkalosis and a high anion gap metabolic acidosis
- However, intubating a patient with salicylate toxicity can reduce minute respiration and lead to respiratory acidosis, masking the respiratory alkalosis and worsening the acidemia
- In some cases, salicylates can interact with laboratory devices which mistakenly read salicylate ions as chloride, leading to falsely elevated chloride levels on the metabolic panel appearing as a normal anion gap metabolic acidosis
- Urinary alkalinization can trap salicylate anions in the renal tubules and promote excretion
- Systemic alkalinization reduces tissue penetration of salicylates
- Hemodialysis is considered for clearance in severe cases:
- Salicylate levels >100 mg/dL or
- Altered mental status
- Hyperthermia
- Non-cardiogenic pulmonary edema
- Cerebral edema
- Seizures
Editors: Jefferson L Triozzi, Payal Gaggar, Joel Topf, Chi Chu, Matthew A. Sparks
Reviewed by: Matthew A. Sparks, M.D, Samira Farouk, M.D, Srinath Yadlapalli, M.D


{kind=link}