Introduction
Kidney transplantation (KT) has been proven to be the optimal form of kidney replacement therapy (KRT) with resultant lower morbidity and mortality rates, and better quality of life.
Why do preemptive kidney transplant recipients have a survival advantage compared to patients getting a transplant after being on dialysis?
Preemptive kidney transplantation (PKT) refers to KT prior to maintenance dialysis initiation. PKT has been proven to be superior to KT done after initiation of chronic dialysis, with PKT recipients having a 5-years survival benefit of up to 10%.
Several studies have shown that the allograft survival benefit in recipients following PKTs stems from patient selection and reduced burden of complications and comorbidities associated with uremia and dialysis, as well as avoidance of access issues and related complications. KTs are also more cost-effective than dialysis, as has been demonstrated that Medicare expenditure on dialysis patients is 2.5 times the expenditure on transplant patients per year based on United States Renal Data Sharing (USRDS) data.
The benefit of PKT was clearly recognized in the “Kidney First Initiative” from 2012, which positioned PKT as the optimal KRT for end stage kidney disease (ESKD). Objective CKD-13.2 in the “Healthy People 2020 initiative” is to “Increase the proportion of patients who receive a preemptive transplant at the start of ESKD”. However, according to USRDS data, in 2017, 86.9% of incident ESRD patients were initiated on HD as their form of KRT, 10.1% started with PD, and only 2.9% received a PKT.
So, Why Do So Few Patients Reap the Benefit of PKTs?
One of the main reasons is that many patients are seen for the first time by a nephrologist when their kidney disease is too advanced to allow enough lag time for referral, work-up, listing, and subsequent PKT, prior to patients requiring initiation of chronic dialysis.
If a living donor is identified during the evaluation and completes all necessary workup, the care team, along with the patient and his family, can aim to schedule a PKT only when the patient’s renal function deteriorates progressively and/or they start exhibiting signs and symptoms of uremia along with persistent metabolic abnormalities.
The optimal timing for PKT remains a controversy. While some believe that when done too early, PKT prevents maximal use of the native kidney function and exposes the recipients and living donors to the risks of operation prematurely, others believe that early restoration of kidney function may slow cardiovascular progression, associated with advanced CKD, thereby decreasing associated morbidity and mortality.
In a study spanning 15 years (1995-2009), it was found a strong trend toward “early” PKT (eGFR>15) over “late” (eGFR<10), in 19,471 PKT recipients. There was no advantage of “early” PKT compared to “late” PKT in terms of graft function, survival, and patient survival.
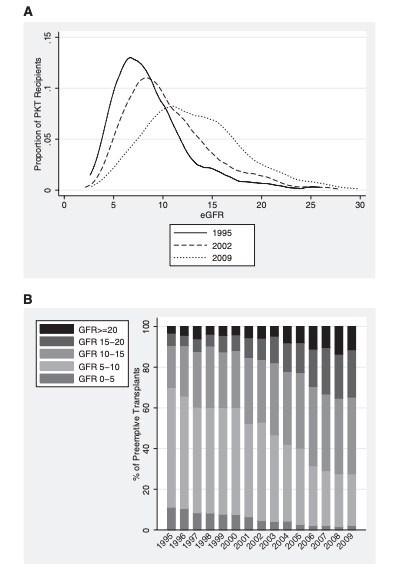
Panel A shows the eGFR distribution between 1995, 2002 and 2009 among patients receiving PKT. Panel B shows the distribution of PKTs based on eGFR categories. Taken together, this data suggests that the timing of PKT has changed, and in recent decades more PKTs are being done earlier (ie – higher eGFR). Reference: Morgan E. Grams, et al; Trends in the Timing of Preemptive Kidney Transplantation. Journal of the American Society of Nephrology. 2011 Sep; 22(9): 1615–1620
It is safe to assume that for potential deceased donor PKTs, given the organ shortage and prolonged waiting time, most patients will experience a period of dialysis pre-transplant even if listed preemptively. However, these patients will likely have a substantially less time on dialysis, thereby maintaining some of the survival benefit associated with PKT.
Implementation of the Kidney Allocation System (2014)
In 2014, the new kidney allocation system (KAS) was introduced, with hopes of solving some of the racial and socio-economic disparities which were observed in access to KT within certain groups such as Hispanics and non-Hispanic blacks . In the year prior to the implementation of KAS, 8.7% of the total number of DDKTs were done preemptively. In the first year after KAS, this number dropped to 5.7% of KTs. This decrease may be related to the large number of patients who were on the waiting list and received wait-time credittimeredit for their time on dialysis (regardless of when they were referred for transplantation) after KAS implementation.
Several studies following the new KAS have shown some improvement of long-standing disparities in listing, however equity of access to KT in general, and to PKT remains an issue. A large observational study compared data before and after the new KAS. Between 2015-2018, 9.8% of DDKT were PKTs, compared to 9% in the years 2000-2013. This mild increase in the proportion of patients receiving PKT was mainly attributed to an increased rate of PKT among white recipients and significant geographical variations on the waiting-time limit the potential expansion of pre-emptive deceased transplants..
Furthermore, adjusted comparative analysis revealed persistence disparities in access to PKT. Non-white, younger patients, males, lower education, and non-private insurance, all had a lower probability of having PKT. Additionally, the median time on the DD waiting list for potential PKT recipients increased, as for patients on dialysis, the “waitlist clock” now starts upon dialysis initiation.
What Lies Ahead
On July 10th, 2019, the White House issued an Executive Order aimed at improving access to KTs, increasing the number of incident ESKD patients receiving a KT and calling for doubling the number of available kidneys by 2030. HHS Launches ‘Advancing American Kidney Health’ Initiative.
As nephrologists, our aim should be that every patient who would benefit from KT would get one in due time, regardless of their gender, race or zip code. Initiatives such as the ‘Advancing American Kidney Health’ Executive Order, along with better education of the natural history of kidney disease and options of kidney replacement therapy for primary physicians, general nephrologists, and the US population at large, can hopefully increase awareness of CKD and ESKD, and lead to an increase in PKT which is the preferred form of kidney transplantation as it has been proven to have better patient and allograft survival.
Goni Katz-Greenberg, MD
Transplant Nephrology Fellow
Thomas Jefferson University Hospital

