A 46 year old man with a recent diagnosis of acute leukemia
and white count of 90,000 was transferred to our facility with non-oliguric AKI
secondary to tumor lysis syndrome. The patient was hypocalcemic (Ca 5.2mg/dl)
and hyperphosphatemic (PO4 11 mg/dl). His K was 5.8 mmol/L and his creatinine
was 3.5 mg/dl. He was making around 200mls/hr of urine and he was asymptomatic.
The Hem/Onc resident called nephrology looking for advice about whether or not
the hypercalcemia should be treated and if he would be better off getting D5W
with bicarbonate instead of normal saline.
and white count of 90,000 was transferred to our facility with non-oliguric AKI
secondary to tumor lysis syndrome. The patient was hypocalcemic (Ca 5.2mg/dl)
and hyperphosphatemic (PO4 11 mg/dl). His K was 5.8 mmol/L and his creatinine
was 3.5 mg/dl. He was making around 200mls/hr of urine and he was asymptomatic.
The Hem/Onc resident called nephrology looking for advice about whether or not
the hypercalcemia should be treated and if he would be better off getting D5W
with bicarbonate instead of normal saline.
TLS is a result of rapid and massive breakdown of tumor
cells, either spontaneously or after the initiation of cytoreductive therapy.
Because potassium is stored primarily in the intracellular compartment, its
rapid release into the extracellular compartment during TLS can lead to
hyperkalemia. Similarly, hyperphosphatemia results from a massive release of
intracellularly stored phosphate, that can lead to secondary hypocalcemia. Uric
acid is the end product of the catabolism of purines, which are released from
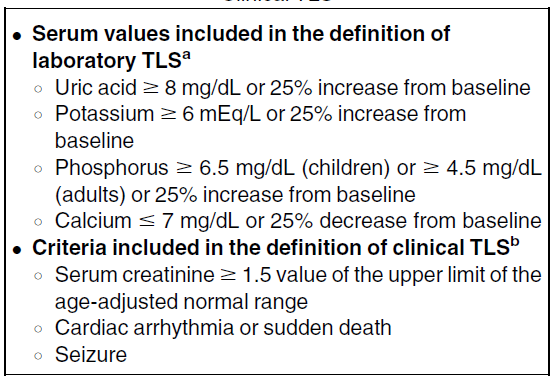
the breakdown of nucleic acids. That lead us to the laboratory definition of
TLS, that was developed by Cairo and Bishop.
cells, either spontaneously or after the initiation of cytoreductive therapy.
Because potassium is stored primarily in the intracellular compartment, its
rapid release into the extracellular compartment during TLS can lead to
hyperkalemia. Similarly, hyperphosphatemia results from a massive release of
intracellularly stored phosphate, that can lead to secondary hypocalcemia. Uric
acid is the end product of the catabolism of purines, which are released from
the breakdown of nucleic acids. That lead us to the laboratory definition of
TLS, that was developed by Cairo and Bishop.
Renal injury can result from two components; the deposition
of uric acid and calcium phosphate crystals, and non-crystal mechanisms
including renal vasoconstriction, alteration in renal autoregulation through
inhibition of nitric oxide synthesis and a resulting decrease in endothelial
cell nitric oxide, and stimulation of the renin-angiotensin system.
of uric acid and calcium phosphate crystals, and non-crystal mechanisms
including renal vasoconstriction, alteration in renal autoregulation through
inhibition of nitric oxide synthesis and a resulting decrease in endothelial
cell nitric oxide, and stimulation of the renin-angiotensin system.
It is best to avoid IV calcium administration unless
hypocalcemia is symptomatic because it might increase the risk of calcium
phosphate precipitation and the potential for additional kidney injury. It is
also best to monitor serum ionized calcium levels, especially in patients with
hypoalbuminemia.
hypocalcemia is symptomatic because it might increase the risk of calcium
phosphate precipitation and the potential for additional kidney injury. It is
also best to monitor serum ionized calcium levels, especially in patients with
hypoalbuminemia.
When rasburicase is available, hyperuricemia is seldom an
indication for dialysis. Rasburicase is a recombinant urate oxidase that
converts uric acid to the more water-soluble product allantoin (which is not
dependent on urinary pH for its solubility).
indication for dialysis. Rasburicase is a recombinant urate oxidase that
converts uric acid to the more water-soluble product allantoin (which is not
dependent on urinary pH for its solubility).
Uric acid solubility is low and increases as urinary pH
becomes more alkaline. However, calcium phosphate is more soluble at an acidic
pH; therefore, urinary alkalinization may lead to increased calcium-phosphate
crystallization and precipitation.
becomes more alkaline. However, calcium phosphate is more soluble at an acidic
pH; therefore, urinary alkalinization may lead to increased calcium-phosphate
crystallization and precipitation.
Therefore, especially when rasburicase is available to
manage the hyperuricemia, urinary alkalinization should be avoided.
manage the hyperuricemia, urinary alkalinization should be avoided.
Going back to the patient, neither Ca nor bicarbonate was
given. Uric acid was not measurable the next day following the use of rasburicase.
PO4 decreased gradually over the next few days, and no dialysis was required
during the hospitalization.
Update: As a commenter pointed out below, rasburicase continues to work in vitro unless the sample is immediately placed on ice and the “undetectable” uric acid level may have been artefactual.
given. Uric acid was not measurable the next day following the use of rasburicase.
PO4 decreased gradually over the next few days, and no dialysis was required
during the hospitalization.
Update: As a commenter pointed out below, rasburicase continues to work in vitro unless the sample is immediately placed on ice and the “undetectable” uric acid level may have been artefactual.
Posted by Tarek Alhamad

Very interesting blog posts! I wanted to introduce you to healthtap.com as a complement to your blog where you can provide personalized answers to real patients about their renal related health questions.
The rasburicase continues to work in the specimen bottle if the secimen is not immediately immersed in ice. That is primarily the reason why uric acid is "undetectable" in most specimens following rasburicase administration.
There are a few typos in this post.