 In 2003, the Fistula First Initiative was enacted, in which an attempt is actively being made to get as many dialysis patients as possible to get dialyzed via an AV fistula. As AV fistulas have been perceived to be the optimal form of dialysis access (with the longest life and fewest infectious complications), this policy seemed to make sense.
In 2003, the Fistula First Initiative was enacted, in which an attempt is actively being made to get as many dialysis patients as possible to get dialyzed via an AV fistula. As AV fistulas have been perceived to be the optimal form of dialysis access (with the longest life and fewest infectious complications), this policy seemed to make sense.
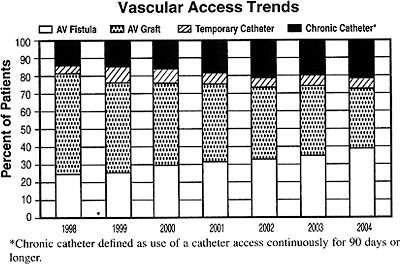 The reason for the increased use of catheters likely stems from the fact that there is an increasing rate of primary fistula failure–typically caused by failure to mature or thrombosis, possibly related to a sicker, more vasculopathic, aging population–and the decreased use of AV grafts. A recent KDOQI workgroup in 2006 re-emphasized that the goal of the Fistula First campaign should be a functional AV fistula, not simply the insertion of an AV fistula with a poor chance at maturing. As one vasscular surgeon at our hospital points out, the initiative should be “Patient First” rather than simply “Fistula First.” In other words, the vascular access strategy should be individualized to the patient–meaning that for elderly, vasculopaths with poor native vessels who are anticipated to require dialysis in the near future, it may be appropriate to begin with a AV graft rather than attempting an AV fistula with little chance of success.
The reason for the increased use of catheters likely stems from the fact that there is an increasing rate of primary fistula failure–typically caused by failure to mature or thrombosis, possibly related to a sicker, more vasculopathic, aging population–and the decreased use of AV grafts. A recent KDOQI workgroup in 2006 re-emphasized that the goal of the Fistula First campaign should be a functional AV fistula, not simply the insertion of an AV fistula with a poor chance at maturing. As one vasscular surgeon at our hospital points out, the initiative should be “Patient First” rather than simply “Fistula First.” In other words, the vascular access strategy should be individualized to the patient–meaning that for elderly, vasculopaths with poor native vessels who are anticipated to require dialysis in the near future, it may be appropriate to begin with a AV graft rather than attempting an AV fistula with little chance of success.
