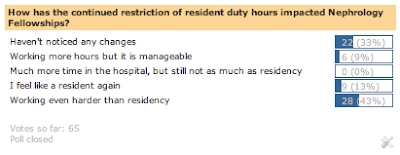
I recently admitted a dialysis patient to a general medicine service for shortness of breath. When receiving signout from the ED resident, she told me that his troponin T was elevated, but since he had had prior high troponin levels, she was not concerned. I decided to do a quick review on troponin levels in dialysis patients in order to help me assess the patient’s cardiovascular risk.
Two main isoforms of troponin are currently used in hospital laboratory assays: troponin T (TnT) and troponin I (TnI). Both are extremely sensitive and specific markers of cardiac ischemia. However, they differ in size and response of serum levels to dialysis. Troponin T is a 37 kDa protein that is elevated in between 30 and 85% of ESRD patients. It is poorly dialyzed, and is cleared by the reticuloendothelial system. TnT levels are either unchanged or increased after dialysis (perhaps because of HD-induced cardiac damage?) Troponin I is a 22 kDa protein integral to the cardiac myocyte contraction apparatus. It is also poorly dialyzed; however, TnI levels usually decrease or remain the same after dialysis. TnI is less frequently elevated in the dialysis population: between 5 and 18% of HD patients exhibit chronically elevated levels. Although troponin levels do associate with renal function, given the size of the proteins, it is thought that increased levels are not related to renal filtration, but instead are secondary to myocardial damage. In support of this notion was a study analyzing troponin levels in transplant patients, which found that Tn did not fall after ESRD patients with elevated troponins were transplanted.
While levels of both troponin isoforms can be elevated in dialysis patients, higher levels have been shown to have prognostic importance. One meta-analysis showed that ESRD patients with elevated TnT had a 2- to 3-fold increased risk of all-cause and cardiac mortality; TnI elevations were also associated with increased mortality risk, although data were more difficult to interpret. TnT levels have also been shown to correlate with CAD disease burden. Although not yet standard of practice, the most recent KDOQI guidelines suggest that “a credible case can be made for recommending the measurement of serum cardiac troponins in dialysis patients for the purpose of risk stratification”.
How useful are elevated troponin levels in predicting acute MI in dialysis patients? Given the percentage of ESRD patients with chronically elevated troponin T, using TnT alone as a marker for acute myocardial damage will lead to some false positives. Because TnI is less often elevated in dialysis patients, it may be more useful for diagnosing acute events. However, given the prognostic significance of elevated troponin levels, any elevation should be taken seriously in symptomatic patients, even if prior levels have also been high. In the case of my patient, his high troponin levels should have been anything but reassuring.
I think the predictive value of troponin T regardless of GFR emphasizes that trop levels are reflective of cardiac damage, not renal function. Elevated trops are associated with ESRD because dialysis patients have a high prevalence of heart disease, not because their kidney function is poor.
What about third generation cardiac troponin T assays as a reliable independent predictor of mortality at all levels of GFR ?
I find the delta-troponin useful in patients with chronically elevated troponins, such as patients with ESRD, as well as patients borderline normal levels but have a high pre-test probability for ischemia or MI. This involves measuring a second troponin about 3 hours after the first draw to see if there is a rise. If the patient is having an acute event that is presumably an NSTEMI, there should be a delta.