 We heard a very interesting presentation today on autoimmune pancreatitis and concurrent systemic disease. The pathogenesis is felt to be related to IgG-4 producing plasma cells, and has now been linked to numerous systemic disease manifestations. The case in question had possible associated autoimmune hypophysitis, leading to presentation with a central diabetes insipidus picture.
We heard a very interesting presentation today on autoimmune pancreatitis and concurrent systemic disease. The pathogenesis is felt to be related to IgG-4 producing plasma cells, and has now been linked to numerous systemic disease manifestations. The case in question had possible associated autoimmune hypophysitis, leading to presentation with a central diabetes insipidus picture.
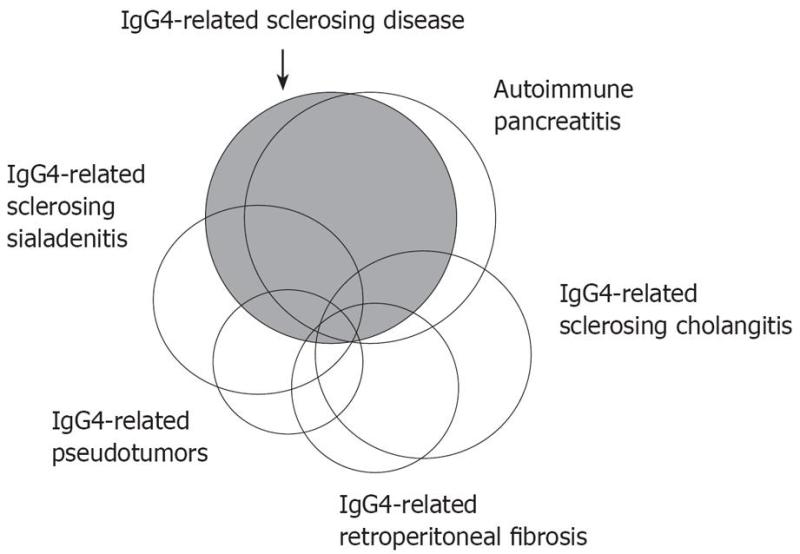
These conditions first came to light following the description of autoimmune pancreatitis and recognition of the association of this disease with various other organ system involvement. The lesions in the affected areas had in common a dense infiltration of IgG-4 plasma cells and T lymphocytes. Involvement has been described in the liver, pancreas, gallbladder, kidneys, retroperitoneum and salivary glands as well as many other tissues.
In terms of renal involvement, the most commonly reported lesion is that of tubulointerstitial nephritis, again with a characteristic infiltration of IgG-4 positive plasma cells. Nodular lesions have also been described, which in many cases can be confusing for primary or secondary malignancies. Of note, sometimes these lesions can be FDG avid, and light up on PET scans, further confusing the picture with malignancy. Membranous nephropathy with IgG-4 positive deposits has also been described. Finally, retroperitoneal fibrosis may also predispose to obstructive nephropathy.
Diagnosis involves biopsy of the affected tissue with demonstration of IgG-4 positive plasma cells. Serum IgG-4 levels should also be requested and, if elevated, have a sensitivity for disease presence of ~70-95%.
Most successful reported treatments have been with corticosteroids, usually starting high and tapering to a lower maintenance dose. There is limited experience in relation to the duration of treatment with steroids or use of steroid-sparing agents in this condition.