To answer this question researchers in Italy took patients from two clinical trials who had serial measured GFR for up to 8 years and compared the results with simultaneous estimates of GFR using the 14 different equations. Of the 600 patients included, 15% were hyperfiltering and 13% had a reduced GFR. Overall, all but one of the equations underestimated GFR in the group as a whole. The single equation that overestimated GFR (Ibrahim) tended to overestimate at all levels. The range of differences between the mGFR and eGFR was -40 to +20 ml/min/1.73m2 and the mean percent error (MPE) ranged from -28.14 to 0.98%. Not unexpectedly, the majority of the error was related to underestimation of GFR in patients with hyperfilatration (MPE -12.8 to -36.7%). It is notable that the MPE was lowest in participants with hyperfiltration using the CKD-Epi equation. In this group, the mean mGFR was 132 ml/min/1.73m2 while the mean eGFR ranged from 83-114 ml/min/1.73m2.
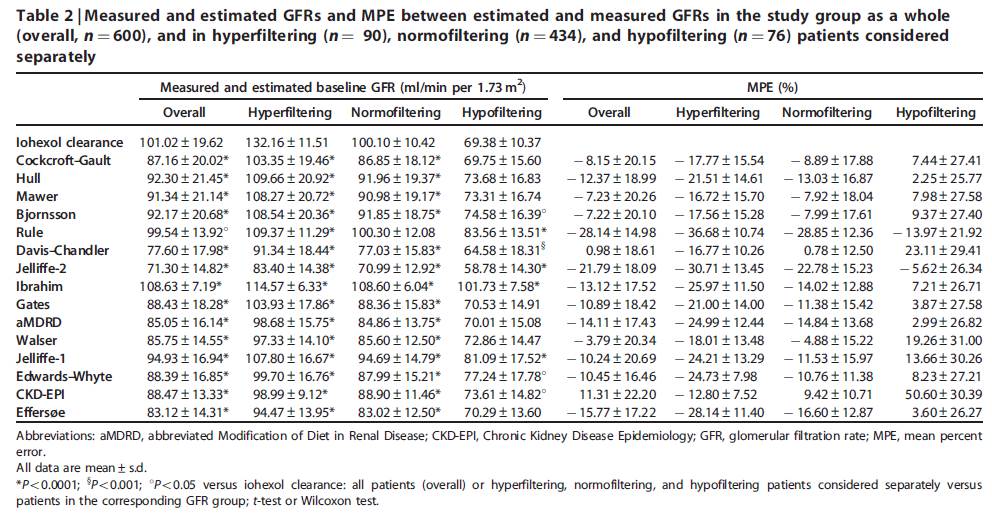
The bias was far lower for the normofiltration and low GFR groups. Because the authors had longitudinal data also, they were able to look at the ability of the formulas to measure GFR decline over time. Given that all of the equations underestimated GFR at baseline, it is unsurprising that there was systematic underestimation of GFR decline over time, particularly in the patients with hyperfiltration. This was less marked in the patients with CKD at baseline. Five of the equations actually estimated that GFR was increasing in the patients despite a consistent decline in mGFR.

This is all not to say that these formulas are not useful. It is always important to recognize the limitations of your tools and one of the major issues here is that creatinine is used as the marker of kidney function with all of the limitations that this introduces. It should also be said that although the agreement with mGFR might not be great, we know from large EPI studies that an eGFR of less than 60 ml/min/1.73m2 is associated with poorer outcomes and this is true no matter what the cause of the disease. The take home from this is that it is not possible to accurately diagnose hyperfiltration in diabetic patients without over nephropathy using current creatinine-based estimating equations and that other signs should be taken into account when assessing these patients.
(Click on images to enlarge)

