I recently managed an elderly African American man who was
admitted from the clinic for a renal biopsy. He was referred for proteinuria
that had not been quantified by his PCP but had been present for over a decade.
His creatinine had risen to 6.8mg/dl from 1.3mg/dl 8 months prior to referral.
His admission UA had no casts, 1 rbc/hpf, 10 wbc/hpf and he had 1.2 g/24hr of
proteinuria. This patient was well with no recent medication changes, NSAID use
or allergies. He was normotensive and had no rash, organomegaly or
lymphadenopathy. Work up was remarkable for slightly positive ANA (1:40), an amylase
of 140U/l and elevated total IgG of 3000mg/dl. He also had elevated white cells
with 79% lymphocytes. His renal ultrasound was normal. Hepatitis serology, HIV,
complement and SPEP were all normal. He had a renal biopsy and a bone marrow
biopsy.
admitted from the clinic for a renal biopsy. He was referred for proteinuria
that had not been quantified by his PCP but had been present for over a decade.
His creatinine had risen to 6.8mg/dl from 1.3mg/dl 8 months prior to referral.
His admission UA had no casts, 1 rbc/hpf, 10 wbc/hpf and he had 1.2 g/24hr of
proteinuria. This patient was well with no recent medication changes, NSAID use
or allergies. He was normotensive and had no rash, organomegaly or
lymphadenopathy. Work up was remarkable for slightly positive ANA (1:40), an amylase
of 140U/l and elevated total IgG of 3000mg/dl. He also had elevated white cells
with 79% lymphocytes. His renal ultrasound was normal. Hepatitis serology, HIV,
complement and SPEP were all normal. He had a renal biopsy and a bone marrow
biopsy.
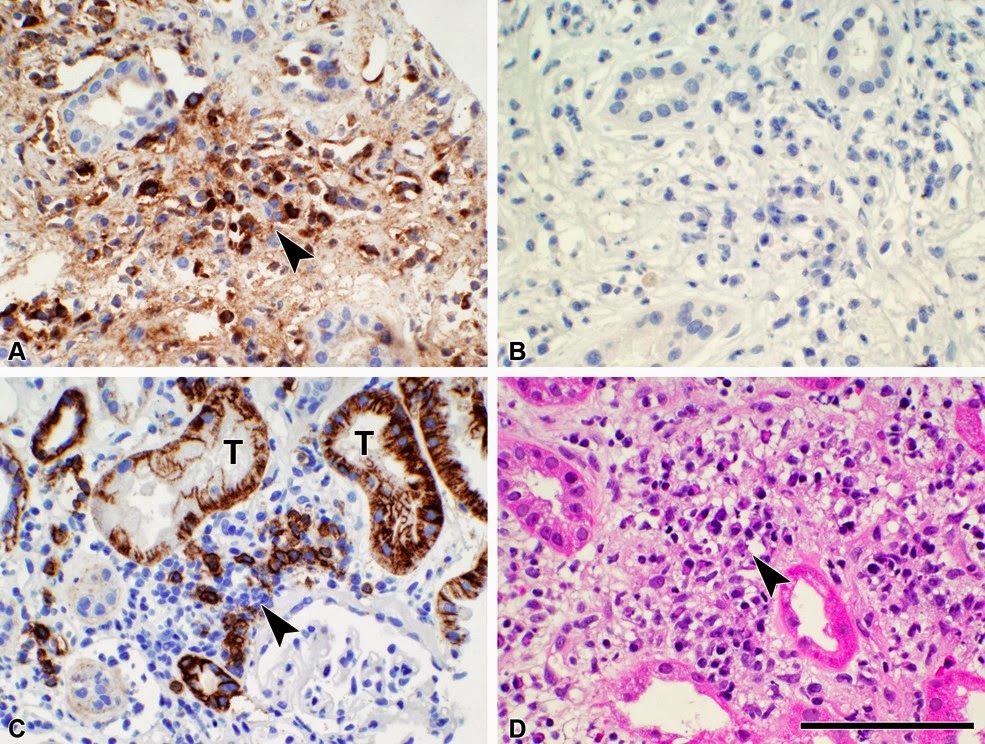
Biopsy findings. In
panel A (immunoperoxidase stain for IgG4), numerous immunoreactive cells are
present (arrowhead). There is also mild,
patchy background staining, not seen in a serial negative control section
(panel B); this may reflect the presence of interstitial IgG4 secreted by the infiltrating
plasma cells. The plasma cells are also
seen in sections stained for CD138 (panel C) and with hematoxylin and eosin
(panel D)(arrowheads). In panel C, there
is also staining for CD138 in the epithelium of proximal tubules (T), which are
known to express the antigen.
panel A (immunoperoxidase stain for IgG4), numerous immunoreactive cells are
present (arrowhead). There is also mild,
patchy background staining, not seen in a serial negative control section
(panel B); this may reflect the presence of interstitial IgG4 secreted by the infiltrating
plasma cells. The plasma cells are also
seen in sections stained for CD138 (panel C) and with hematoxylin and eosin
(panel D)(arrowheads). In panel C, there
is also staining for CD138 in the epithelium of proximal tubules (T), which are
known to express the antigen.
This patient was diagnosed with IgG4-Tubulointerstial
Nephritis and also with CLL after his bone marrow biopsy. He was treated with
60mg of prednisone for his IgG4-TIN and his creatinine improved to 2.7mg/dl within
a month. He was tapered off steroids over months and his eGFR remains at about
30ml/min/1.73m2.
Nephritis and also with CLL after his bone marrow biopsy. He was treated with
60mg of prednisone for his IgG4-TIN and his creatinine improved to 2.7mg/dl within
a month. He was tapered off steroids over months and his eGFR remains at about
30ml/min/1.73m2.
IgG4 related systemic disease was first described in
pancreatic specimens that had been removed for suspected malignancy found on
imaging. Now it is known that this inflammatory condition can affect many
organs including the kidney. The most common renal lesion is infiltration of
the interstitium with IgG4 positive plasma cells but other lesions such as
membranous nephropathy can occur. Abnormal radiological findings in the kidney
also occur. The full diagnostic criteria proposed by Raisson et al is shown
here.
pancreatic specimens that had been removed for suspected malignancy found on
imaging. Now it is known that this inflammatory condition can affect many
organs including the kidney. The most common renal lesion is infiltration of
the interstitium with IgG4 positive plasma cells but other lesions such as
membranous nephropathy can occur. Abnormal radiological findings in the kidney
also occur. The full diagnostic criteria proposed by Raisson et al is shown
here.
- Histology: >10 IgG4 positive plasma cells/hpf in the most concentrated field (mandatory) and tubular basement membrane immune complex deposition by IF, IHC and/or EM (supportive, present in >80% of cases)
- Imaging: Small cortical nodules, round or wedge lesions and/or enlargement of the kidneys
- Serology: elevated serum IgG4 or total IgG
- Other organ involvement such as autoimmune pancreatitis or lymphadenopathy
IgG4-TIN is diagnosed when (1) is present plus one of the features described in (2)-(4)
In this month’s KI issue Saeki et al report on the long term
follow up of 43 patients with IgG4-related kidney disease (IgG4-TIN) from
Japan. Follow up data on these cases is rare. 34 patients were treated with
corticosteroids and followed for at least 12 months in this study. In summary,
IgG4-TIN is usually responsive to corticosteroid treatment and response is
rapid but not total. If eGFR was lower than 60 before treatment renal scaring
is more likely to occur. Relapse occurs in about 20% but most are responsive to
further steroid treatment. Serological markers and radiological features all
improve with treatment for the most part.
follow up of 43 patients with IgG4-related kidney disease (IgG4-TIN) from
Japan. Follow up data on these cases is rare. 34 patients were treated with
corticosteroids and followed for at least 12 months in this study. In summary,
IgG4-TIN is usually responsive to corticosteroid treatment and response is
rapid but not total. If eGFR was lower than 60 before treatment renal scaring
is more likely to occur. Relapse occurs in about 20% but most are responsive to
further steroid treatment. Serological markers and radiological features all
improve with treatment for the most part.
There are no large-scale studies for this disorder that was
first described with any frequency in Japan. This is a renal condition that is
gaining more and more coverage in the renal literature and any budding
nephrologist needs to be aware of it. Whether this is a new disease or a
disease diagnosed more frequently with the advent of better immunohistochemical
stains for IgG4 is unknown. My feeling is that it is the latter.
first described with any frequency in Japan. This is a renal condition that is
gaining more and more coverage in the renal literature and any budding
nephrologist needs to be aware of it. Whether this is a new disease or a
disease diagnosed more frequently with the advent of better immunohistochemical
stains for IgG4 is unknown. My feeling is that it is the latter.
Posted by Andrew Malone