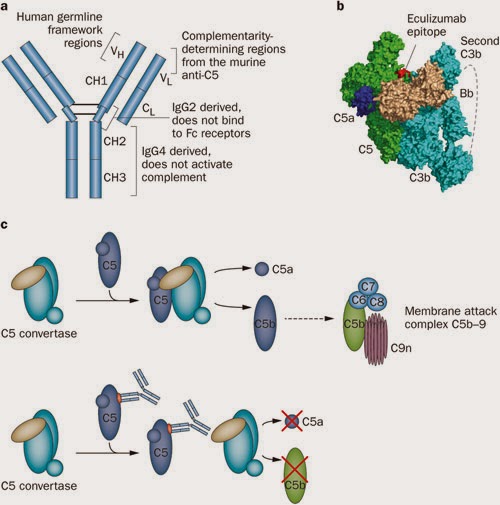
Eculizumab is a humanized monoclonal antibody (mAb) that binds the complement protein C5 blocking its cleavage into C5a and C5b, thereby preventing the formation of the C5b-9, the Membrane Attack Complex (MAC).
Eculizumab is FDA approved for the treatment of paroxysmal nocturnal haemoglobinuria, and for atypical HUS (aHUS).
It has been used off-label in the treatment of TTP refractory to plasmapheresis.
In renal transplant recipients, it has been use, so far, for :
– Treatment of variety of complement/antibody-mediated microangiopathy syndromes such as atypical HUS.
– Severe antibody-mediated rejection (AMR)/Desensitization protocol;
– Patients with Antiphospholipid Antibody Syndrome (APS) and its rare subtype, Catastrophic Antiphospholidid
Antibody Syndrome (CAPS);
-To reverse the potentially fatal effects of graft reperfusion injury
-To rescue Severe Accelerated AMR in ABO incompatible kidney transplant.
In lung transplant recipients to treat:
– aHUS in combined Lung-Kidney transplant.
– Hyperacute AMR
In Bone Marrow transplant patients it has been used to treat severe hematopoietic stem cell transplantation-associated thrombotic microangiopathy (HSCT-TMA).
Few important points:
- It is mandatory for patients to be immunized against meningococcus, hemophilus and pneumococci if not current due to the central role of the complement system in fighting infection. Nonetheless, meningococcal sepsis can be seen despite appropriate vaccination.
- Due to Eculizumab®’s mechanism of action, levels of antibodies-of any kind- are unchanged during its use; therefore researchers are still working to find a way to more accurately measure treatment response.
** More recently, Lonze and Mongomery’s group at Johns Hopkins used a bioassay as a functional measure of complement blockade and investigated the utility of C5b-9 (MAC) staining on kidney and skin biopsies. They demonstrated on prior studies, that skin tissue is an extremity sensitive site for the detection of C5b-9 deposition. They used normal skin biopsy sites prior to transplant in 3 patients with APS as baseline test. The follow up was done with skin and kidney biopsies. Their concluded that finding a progressive decrement in C5b-9 staining was not useful. Mainly, because it takes several months to almost a year for the tissue samples to no longer demonstrate C5b-9 deposition despite the effective blockade of complement almost immediately after the initial administration of the drug. And, of course, the skin biopsies will only be useful on patients with systemic diseases only. Nevertheless, they successfully transplanted 3 patients with APS, 2 of them with CAPS and highly sensitized. The patients continue to have functioning renal allografts while receiving monthly infusions of Eculizumab indefinitely given their livelong risk of thrombotic events and the poor outcome associated with recurrent CAPS episodes in prior case reports on APS patients with anticoagulation alone.
Take home messages:
–Vaccinate patients who potentially will need Eculizumab prior to transplant (at least 4 months).
– The duration of use is still unclear, but some patients with genetic abnormalities in complement activation may need life-long therapy.
-Adjust dose when using plasmapheresis (redosing after pheresis).
-You may need to do transplant kidney biopsies more frequently to follow up histology in cases of desensitization/AMR since currently there is no other more accurate way to find out if the therapy is working.
– Still no long-term safety data available.
Since the variety of complement activation diseases is broad, is not going to be easy to do RTC, and on top of that, placebo arms will be mostly unacceptably in high risk for transplant patients. Nevertheless, large trials are warranted to prove its efficacy and long term safety… stay tune!
Figure from review from Zuber et al. Nat Rev Nephrol 2012
Adela Mattiazzi, MD

