Recently a 65-year-old
female was referred to an ED in the state of Missouri complaining of fevers,
chills, headache, diarrhea and vomiting occurring over the last week. 3 weeks prior
she had received an orthotopic liver transplant. Her post transplant course was
unremarkable and she was discharged on prograf 2mf bid, myfortic 360mg bid,
prednisone tapering, Bactrim single strength daily and valcyte 450mg od. She
also took thyroid replacement, Januvia, warfarin and aspirin. Past medical
history included diabetes, heart failure, dysfunctional uterine bleeding,
hypothyroid and PUD. She also had CKD with a creatinine about 1.4mg/dl. On
examination her Temp was 38.6, HR 110, BP 113/76 and O2sats 99% on RA. She had
no nuchal rigidity but reported a sore neck. She had an erythematous area on
her lower back. The rest of her exam was normal.
were:
(94%neuts, 5.8%lymphs), platelets 35
CO2 20, O2 102
155, GGT 171, Bili 0.6, Alb 3.3
2 rbc, 2 wbc
CT brain and was started on multiple antibiotics in the ED.
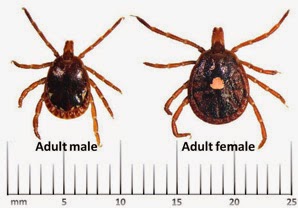
questioning her daughter reported removing a tick from her back after the
patient went out looking at deer close to her house.
daughter brought in a picture of the tick (see above)!
admission to discharge.
was performed.
commenced.
creatinine improved and potassium became low, likely due to GI losses.
leucopenia followed the classical pattern of lymphopenia followed by leucopenia
and she required G-CSF. Her transaminases were normal at the time of discharge.
The first case of
human ehrlichiosis was described in 1986.
important species to infect humans are Ehrlichia chaffeensis which causes human
monocytic ehrlichiosis (HME) and Anaplasma phagocytophilum which causes human
granulocytic anaplasmosis (HGA). Both of these diseases have the same vector
and have very similar clinical and laboratory features. Ehrlichia ewingii is a
less common cause of ehrlichiosis than Ehrlichia chaffeensis.
obligate intracellular bacteria found in membrane bound vacuoles in human and
animal leukocytes.
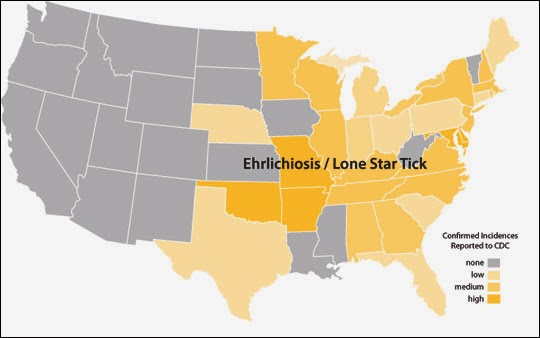
area is the southeastern USA – ‘the tick belt’. See the CDC map for the endemic
regions in the USA. Cases have also been reported in Europe, Africa, South
America and Mexico.
(Amblyomma americanum) is recognized by the CDC as the principal vector of
Ehrlichia chaffeensis and Ehrlichia ewingii in the U.S.; both disease agents
are responsible for causing ehrlichiosis in humans. White-tailed deer are a
primary host of the lone star tick and appear to serve as a natural reservoir
for E. chaffeensis. The lone star tick is also a vector of Francisella
tularensis, causal agent of tularemia. Adult ticks parasistize deer, cattle,
horses, feral swine, sheep, dogs, and humans.
occur in the spring and summer in the USA.
manifestations in the elderly and immunosuppressed can be very severe but the
following are the usual clinical features:
fevers can be protracted over weeks
headache and chills – 2/3
and arthralgia – ¼ to ½
mucopapular, petechial) – 1/3
Seizures, coma, renal failure, heart failure and respiratory failure
single case of myocarditis and multi-organ failure in a healthy adolescent.
findings:
transaminases.
to be caused by lymphopenia initially followed by neutropenia as in this
patient.
transaminases, LDH and Alk phos
creatinine
neurological symptoms
pleocytosis and elevated CSF protein
methods. Note this test may not detect the recently reported third species, E.
muris, found in Wisconsin and Minnesota.
diagnosis
difficult diagnosis to make. It is clinically and geographically similar to
RMSF. It can also present like mononucleosis, TTP, hematologic malignancy,
cholangitis, the early phases of hepatitis A infection. This is especially so
in immunocompromised patients whose clinical features may not be as obvious
initially. Common transplant drugs such as Bactrim/Septra, valganciclovir,
mycophenolate and azathioprine can also cause cytopenias.
iv or po bid for about 10 days.
also treat RMSF which is often confused with ehrlichiosis.
Mortality is about 5%. Most commonly due to viral or fungal super-infections
(Invasive aspergillosis, candida, HSV).
difficulty in diagnosing tick borne infections. They can be lethal and severe
in our immunosuppressed transplant population and can be a cause of renal
failure in any patient. Also of interest in
this case is the lymphocytopenic and neutropenic trending that is usually more
peculiar to Anaplasma phagocytophilum which causes
human granulocytic anaplasmosis (HGA). We did not test for A phagocytophilum as
ehrlichae PCR was positive.
